de Font-Réaulx Enrique, Solis-Santamaria Andrea, Arch-Tirado Emilio, González-Astiazarán Adalberto
Head, Department of Epilepsy Surgery, Neurological Center, Centro Médico ABC, Mexico City, Mexico.
Benemérita Universidad Autónoma de Puebla Medical School, Puebla, Mexico.
Surg Neurol Int. 2024 Mar 1;15:63. doi: 10.25259/SNI_763_2023. eCollection 2024.
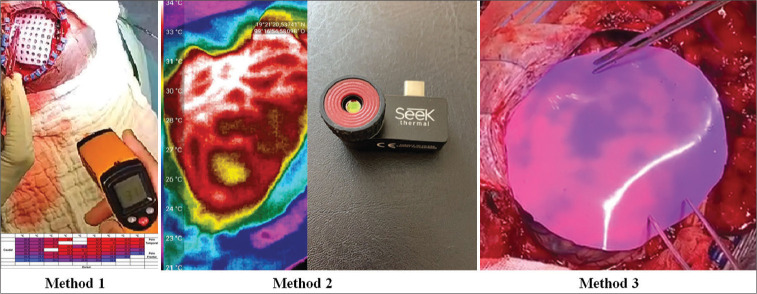
Epilepsy surgery represents a therapeutic opportunity for those patients who do not respond to drug therapy. However, an important challenge is the precise identification of the epileptogenic area during surgery. Since it can be hard to delineate, it makes it necessary to use auxiliary tools as a guide during the surgical procedure. Electrocorticography (ECoG), despite having shown favorable results in terms of reducing post-surgical seizures, have certain limitations. Brain mapping using infrared thermography mapping and a new thermosensitive/thermochromic silicone (TTS) in epilepsy surgery has introduced a new resource of noninvasive and real-time devices that allow the localization of irritative zones.
Sixty consecutive patients with drug-resistant epilepsy with surgical indications who decided to participate voluntarily in the study were included in the study. We measured brain temperature using two quantitative methods and a qualitative method: the TTS sheet. In all cases, we used ECoG as the gold standard to identify irritative areas, and all brain tissue samples obtained were sent to pathology for diagnosis.
In the subgroup in which the ECoG detected irritative areas ( = 51), adding the results in which there was a correlation with the different methods, the efficiency obtained to detect irritative areas is 94.11% ( = 48/51, ≤ 0.0001) while the infrared thermography mapping method independently has an efficiency of 91.66% ( ≤ 0.0001). The TTS has a sensitivity of 95.71% and a specificity of 97.9% ( ≤ 0.0001) to detect hypothermic areas that correlate with the irritative zones detected by ECoG. No postoperative infections or wound dehiscence were documented, so the different methodologies used do not represent an additional risk for the surgical proceedings.
We consider that the infrared thermography mapping using high-resolution infrared thermography cameras and the TTS are both accurate and safe methods to identify irritative areas in epilepsy surgeries.
癫痫手术为那些药物治疗无效的患者提供了一种治疗机会。然而,一个重要的挑战是在手术过程中精确识别致痫区域。由于该区域难以界定,因此在手术过程中需要使用辅助工具作为指导。皮质脑电图(ECoG)尽管在减少术后癫痫发作方面显示出良好效果,但存在一定局限性。在癫痫手术中使用红外热成像图谱和新型热敏/热致变色硅酮(TTS)进行脑图谱绘制,引入了一种非侵入性实时设备的新资源,可实现刺激区域的定位。
本研究纳入了60例连续的有手术指征的耐药性癫痫患者,他们自愿决定参与该研究。我们使用两种定量方法和一种定性方法(TTS片)测量脑温。在所有病例中,我们将ECoG作为识别刺激区域的金标准,并且将获取的所有脑组织样本送去做病理诊断。
在ECoG检测到刺激区域的亚组(n = 51)中,综合与不同方法有相关性的结果,检测刺激区域的效率为94.11%(n = 48/51,P≤0.0001),而红外热成像图谱法单独使用时的效率为91.66%(P≤0.0001)。TTS检测与ECoG检测到的刺激区域相关的低温区域的灵敏度为95.71%,特异性为97.9%(P≤0.0001)。未记录到术后感染或伤口裂开情况,因此所采用的不同方法对手术过程不构成额外风险。
我们认为,使用高分辨率红外热成像相机的红外热成像图谱和TTS都是在癫痫手术中识别刺激区域的准确且安全的方法。