Patterson Benjamin, Dinkele Ryan, Gessner Sophia, Koch Anastasia, Hoosen Zeenat, January Vanessa, Leonard Bryan, McKerry Andrea, Seldon Ronnett, Vazi Andiswa, Hermans Sabine, Cobelens Frank, Warner Digby F, Wood Robin
Amsterdam Institute for Global Health and Development, University of Amsterdam, Amsterdam 1105, The Netherlands.
South African Medical Research Council, National Health Laboratory Service, University of Cape Town Molecular Mycobacteriology Research Unit & Department of Science and Technology/National Research Foundation Centre of Excellence for Biomedical TB Research, Department of Pathology, Faculty of Health Sciences, University of Cape Town, Cape Town 7925, South Africa.
Proc Natl Acad Sci U S A. 2024 Mar 19;121(12):e2314813121. doi: 10.1073/pnas.2314813121. Epub 2024 Mar 12.
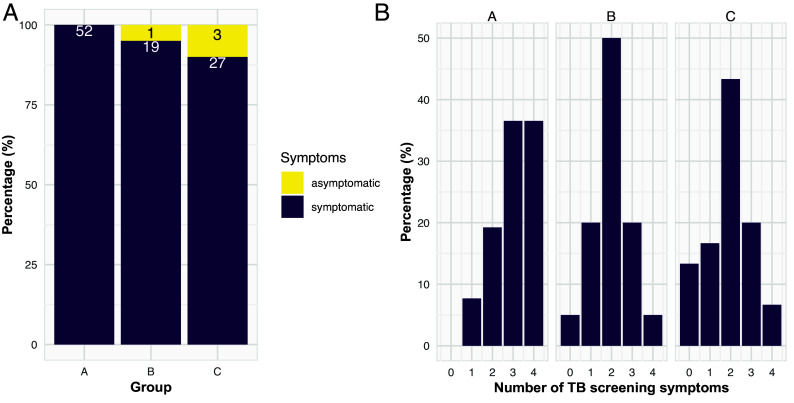
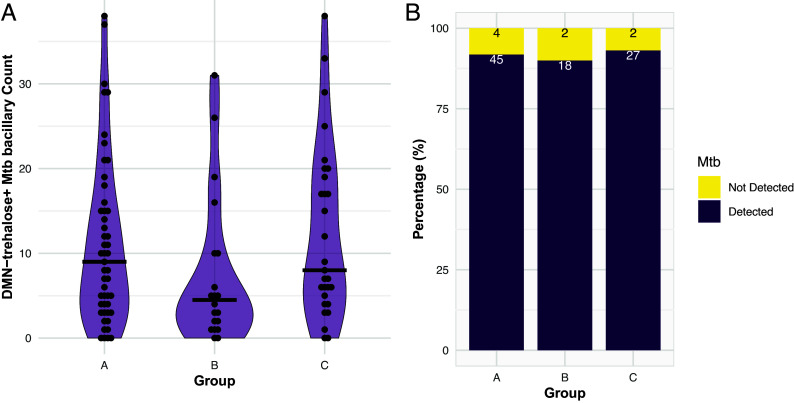
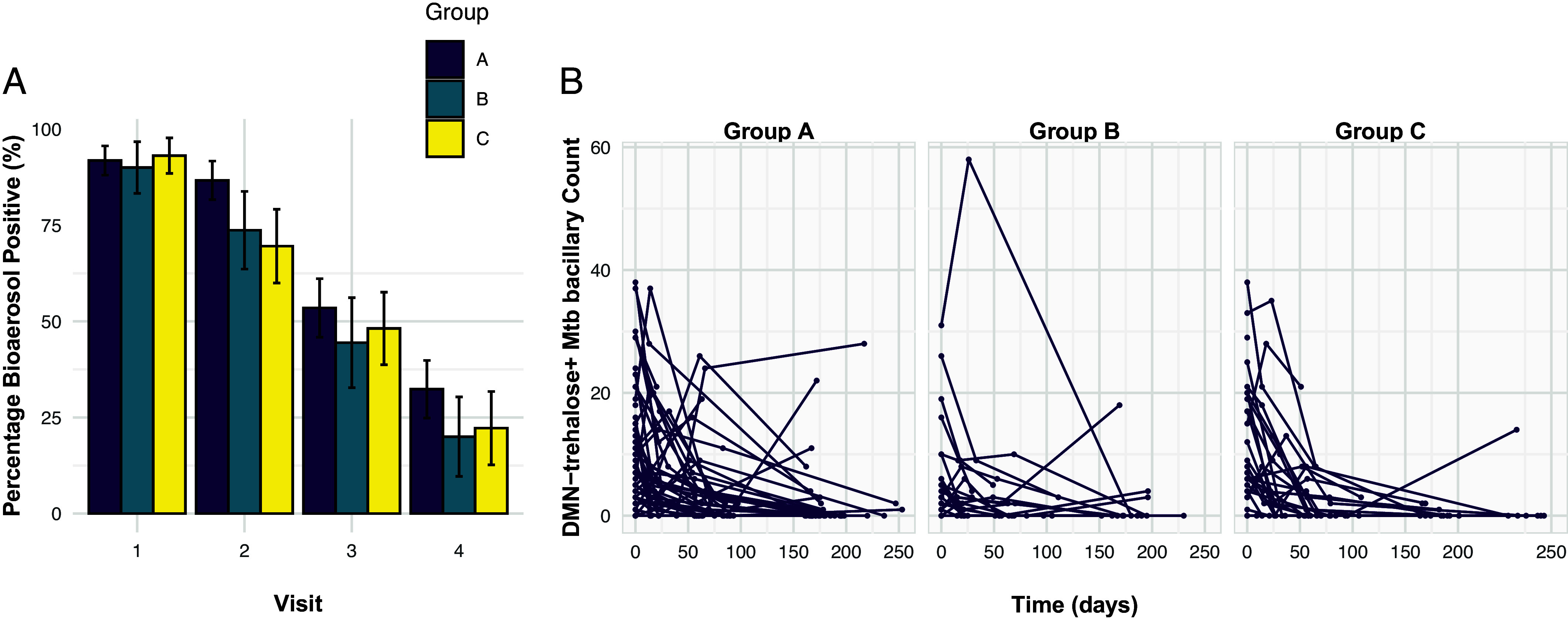
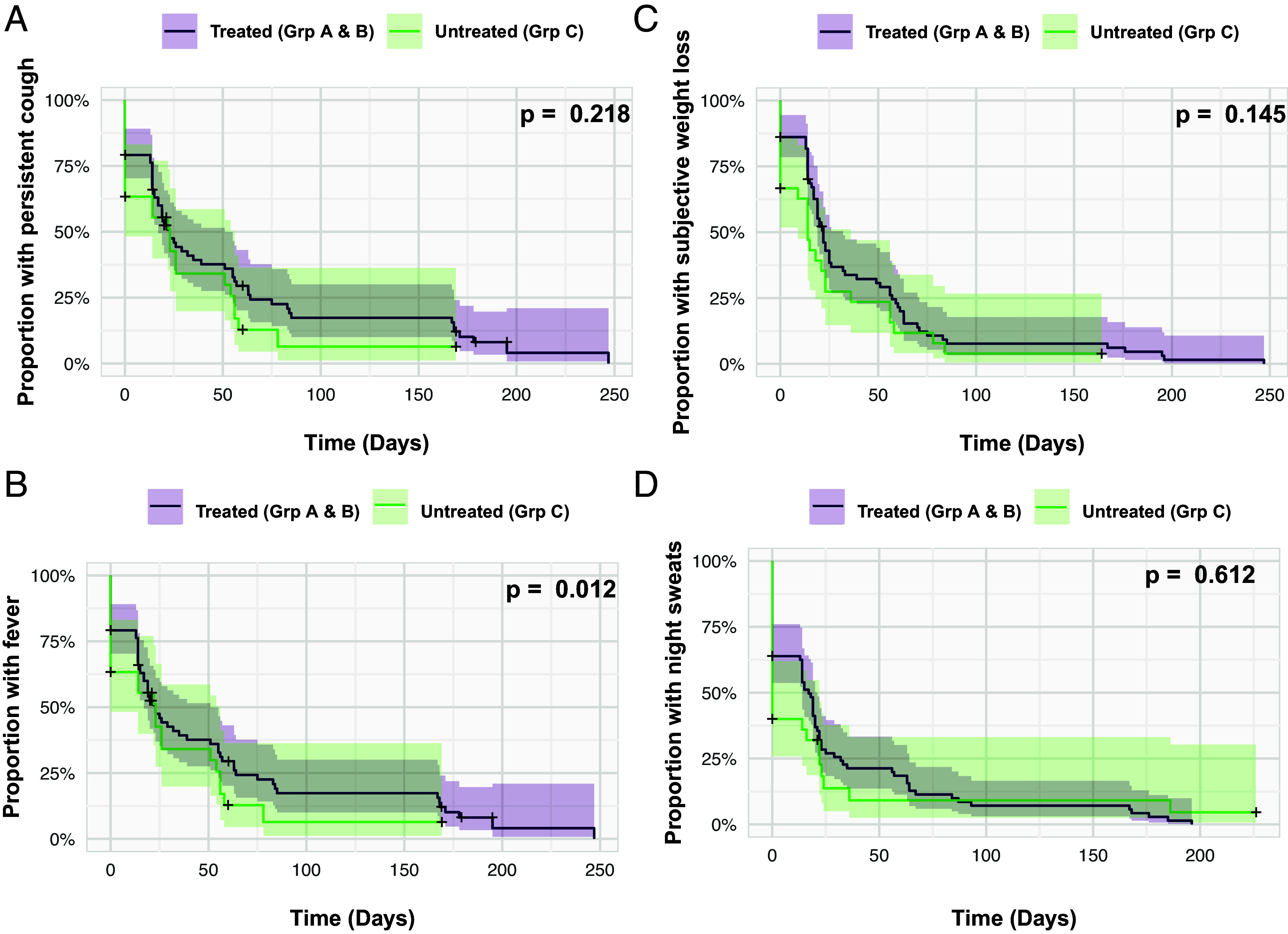
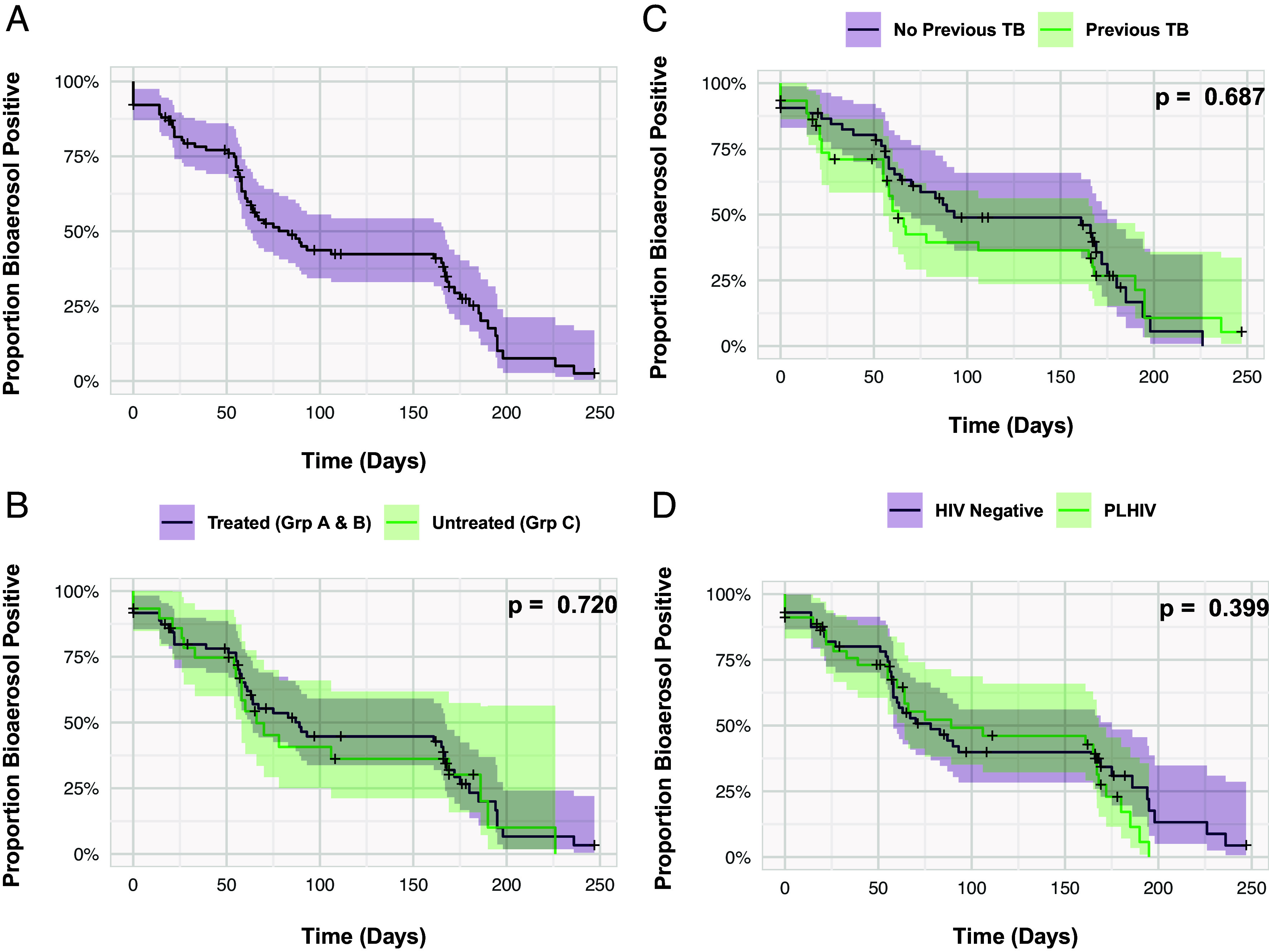
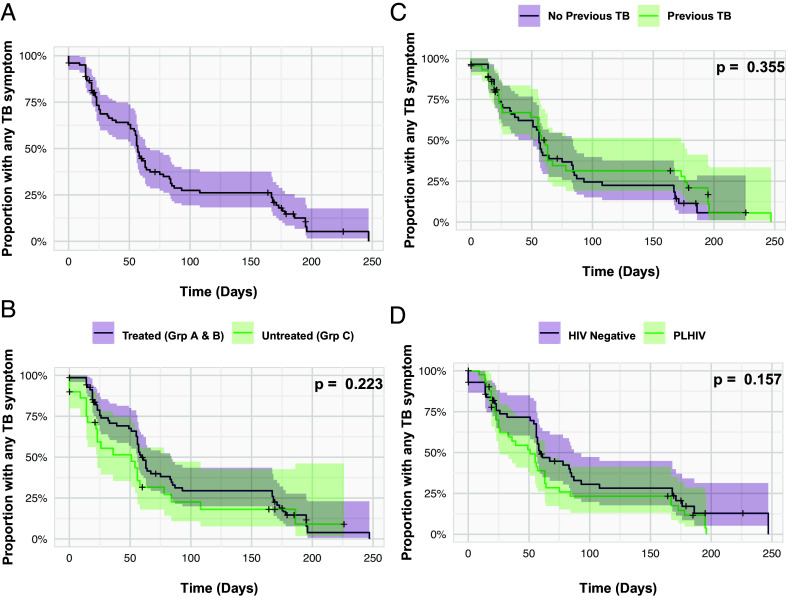
Potential () transmission during different pulmonary tuberculosis (TB) disease states is poorly understood. We quantified viable aerosolized from TB clinic attendees following diagnosis and through six months' follow-up thereafter. Presumptive TB patients (n=102) were classified by laboratory, radiological, and clinical features into Group A: Sputum-Xpert Ultra-positive TB (n=52), Group B: Sputum-Xpert Ultra-negative TB (n=20), or Group C: TB undiagnosed (n=30). All groups were assessed for bioaerosol release at baseline, and subsequently at 2 wk, 2 mo, and 6 mo. Groups A and B were notified to the national TB program and received standard anti-TB chemotherapy; was isolated from 92% and 90% at presentation, 87% and 74% at 2 wk, 54% and 44% at 2 mo and 32% and 20% at 6 mo, respectively. Surprisingly, similar numbers were detected in Group C not initiating TB treatment: 93%, 70%, 48% and 22% at the same timepoints. A temporal association was observed between bioaerosol release and TB symptoms in all three groups. Persistence of bioaerosol positivity was observed in ~30% of participants irrespective of TB chemotherapy. Captured bacilli were predominantly acid-fast stain-negative and poorly culturable; however, three bioaerosol samples yielded sufficient biomass following culture for whole-genome sequencing, revealing two different lineages. Detection of viable aerosolized in clinic attendees, independent of TB diagnosis, suggests that unidentified transmitters might contribute a significant attributable proportion of community exposure. Additional longitudinal studies with sputum culture-positive and -negative control participants are required to investigate this possibility.
不同肺结核(TB)疾病状态下潜在的()传播情况尚不清楚。我们对结核病门诊患者诊断后及随后六个月随访期间可存活的雾化()进行了定量分析。根据实验室、放射学和临床特征,将疑似结核病患者(n = 102)分为A组:痰Xpert Ultra阳性结核病(n = 52)、B组:痰Xpert Ultra阴性结核病(n = 20)或C组:未确诊结核病(n = 30)。在基线时以及随后的第2周、第2个月和第6个月对所有组进行生物气溶胶释放评估。A组和B组被通报给国家结核病项目并接受标准抗结核化疗;就诊时分别从92%和90%的患者中分离出(),第2周时分别为87%和74%,第2个月时分别为54%和44%,第6个月时分别为32%和20%。令人惊讶的是,在未开始抗结核治疗的C组中检测到的数量相似:在相同时间点分别为93%、70%、48%和22%。在所有三组中均观察到生物气溶胶释放与结核症状之间存在时间关联。无论是否进行抗结核化疗,约30%的参与者中观察到生物气溶胶阳性持续存在。捕获的()杆菌主要为抗酸染色阴性且难以培养;然而,三个生物气溶胶样本在培养后产生了足够的生物量用于全基因组测序,揭示了两种不同的()谱系。在门诊患者中检测到可存活的雾化(),与结核病诊断无关,这表明未识别的()传播者可能在社区暴露的可归因比例中占很大一部分。需要对痰培养阳性和阴性对照参与者进行额外的纵向研究来调查这种可能性。