Koltenyuk Victor, Mrad Ismat, Choe Ian, Ayoub Mohamad Ibrahim, Kumaraswami Sangeeta, Xu Jeff L
School of Medicine, New York Medical College, Valhalla, NY, USA.
Anesthesiology and Perioperative Medicine, University of Rochester, Rochester, NY, USA.
J Pain Res. 2024 Feb 29;17:797-813. doi: 10.2147/JPR.S434010. eCollection 2024.
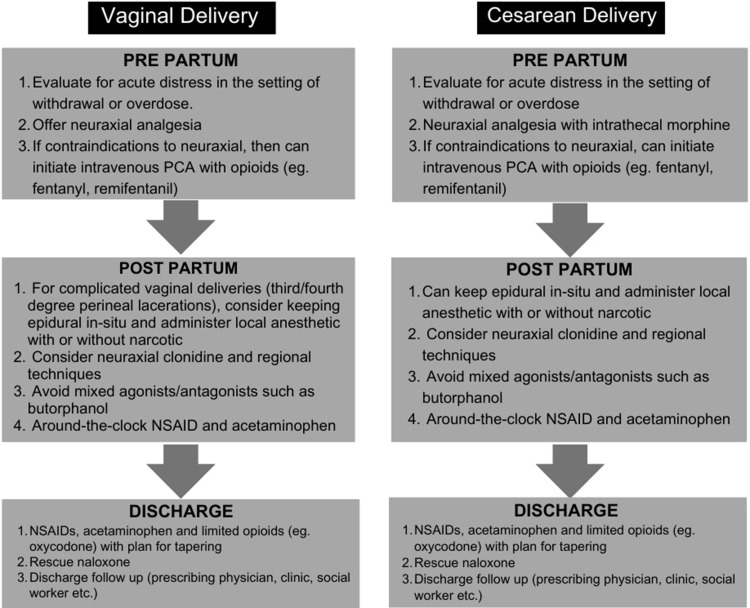
The opioid epidemic in the United States has led to an increasing number of pregnant patients with opioid use disorder (OUD) presenting to obstetric units. Caring for this complex patient population requires an interdisciplinary approach involving obstetricians, anesthesiologists, addiction medicine physicians, psychiatrists, and social workers. The management of acute pain in the parturient with OUD can be challenging due to several factors, including respiratory depression, opioid tolerance, and opioid-induced hyperalgesia. Patients with a history of OUD can present in one of three categories: 1) those with untreated OUD; 2) those who are currently abstinent from opioids; 3) those being treated with medications to prevent withdrawal. A patient-centered, multimodal approach is essential for optimal peripartum pain relief and prevention of adverse maternal and neonatal outcomes. Medications for opioid use disorder (MOUD), previously referred to as medication-assisted therapy (MAT), include opioids like methadone, buprenorphine, and naltrexone. These are prescribed for pregnant patients with OUD, but appropriate dosing and administration of these medications are critical to avoid withdrawal in the mother. Non-opioid analgesics such as acetaminophen and nonsteroidal anti-inflammatory drugs (NSAIDs) can be used in a stepwise approach, and regional techniques like neuraxial anesthesia and truncal blocks offer opioid-sparing options. Other medications like ketamine, clonidine, dexmedetomidine, nitrous oxide, and gabapentinoids show promise for pain management but require further research. Overall, a comprehensive pain management strategy is essential to ensure the well-being of both the mother and the fetus in pregnant patients with OUD.
美国的阿片类药物流行导致越来越多患有阿片类药物使用障碍(OUD)的孕妇前往产科病房。照顾这一复杂的患者群体需要一种跨学科方法,涉及产科医生、麻醉医生、成瘾医学医生、精神科医生和社会工作者。由于多种因素,包括呼吸抑制、阿片类药物耐受性和阿片类药物诱导的痛觉过敏,患有OUD的产妇急性疼痛的管理可能具有挑战性。有OUD病史的患者可分为三类:1)未治疗的OUD患者;2)目前已戒除阿片类药物的患者;3)正在接受药物治疗以预防戒断症状的患者。以患者为中心的多模式方法对于实现最佳围产期疼痛缓解以及预防不良母婴结局至关重要。用于治疗阿片类药物使用障碍(MOUD)的药物,以前称为药物辅助治疗(MAT),包括美沙酮、丁丙诺啡和纳曲酮等阿片类药物。这些药物用于患有OUD的孕妇,但这些药物的适当剂量和给药对于避免母亲出现戒断症状至关重要。对乙酰氨基酚和非甾体抗炎药(NSAIDs)等非阿片类镇痛药可以逐步使用,而神经轴麻醉和躯干阻滞等区域技术提供了减少阿片类药物使用的选择。氯胺酮、可乐定、右美托咪定、氧化亚氮和加巴喷丁类药物等其他药物在疼痛管理方面显示出前景,但需要进一步研究。总体而言,全面的疼痛管理策略对于确保患有OUD的孕妇的母亲和胎儿的健康至关重要。