Biostatistics, Epidemiology and Public Health Research Team, Department of Statistics, Shahjalal University of Science and Technology, Sylhet, Bangladesh.
Department of Geography and Environment, Shahjalal University of Science and Technology, Sylhet, Bangladesh.
PLoS One. 2024 Mar 21;19(3):e0300347. doi: 10.1371/journal.pone.0300347. eCollection 2024.
Antimalarial drug resistance poses a severe danger to global health. In Low- and Middle-Income Countries (LMICs), there is a lack of reliable information on antimalarial prescriptions for recent malarial fever in children under five. Our study aims to determine the prevalence of unqualified sources of antimalarial drug prescription for children under the age of five in 19 low- and middle-income countries.
We performed a cross-sectional study of the Malaria Indicator Survey (MIS) datasets (n = 106265) across 19 LMICs. The recent MIS datasets were used, and the study only included children under five who had taken an antimalarial drug for a recent malarial fever. The outcome variable was classified into two distinct categories: those who had taken antimalarial drugs for malarial fever from qualified sources and those who did not.
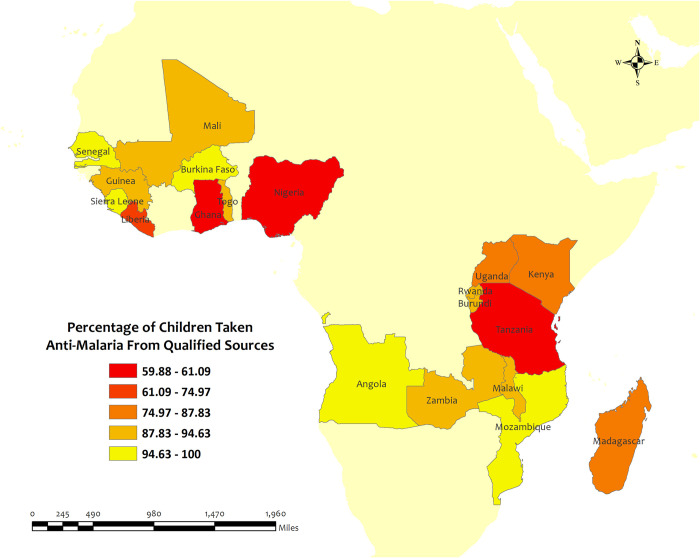
Among LMICs, we found that 87.1% of children under five received an antimalarial prescription from unqualified sources who had recently experienced malarial fever. In several LMICs (Tanzania, Nigeria, and Ghana), a substantial portion of recent antimalarial prescriptions for malaria was taken from unqualified sources (about 60%). Some LMICs (Guinea (31.8%), Mali (31.3%), Nigeria (20.4%), Kenya (2.6%), and Senegal (2.7%)) had low rates of antimalarial drug consumption even though children under five received a high percentage of antimalarial prescriptions from qualified sources for a recent malarial fever. Living in rural areas, having mothers with higher education, and having parents with more wealth were frequently taken antimalarial from qualified sources for recent malarial fever in children under five across the LMICs.
The study draws attention to the importance of national and local level preventative strategies across the LMICs to restrict antimalarial drug consumption. This is because antimalarial prescriptions from unqualified sources for recent malarial fever in children under five were shockingly high in most LMICs and had high rates of unqualified prescriptions in certain other LMICs.
抗疟药物耐药性对全球健康构成严重威胁。在中低收入国家(LMICs),缺乏关于最近五岁以下儿童疟疾发热的抗疟处方的可靠信息。我们的研究旨在确定 19 个中低收入国家最近五岁以下儿童抗疟药物处方不合格来源的流行率。
我们对 19 个 LMICs 的疟疾指标调查(MIS)数据集(n=106265)进行了横断面研究。使用最近的 MIS 数据集,仅包括因最近疟疾发热而服用抗疟药物的五岁以下儿童。因变量分为两类:从合格来源服用抗疟药物治疗疟疾发热的儿童和未服用抗疟药物的儿童。
在 LMICs 中,我们发现 87.1%的最近因疟疾发热服用抗疟药物的五岁以下儿童来自不合格来源。在几个 LMICs(坦桑尼亚、尼日利亚和加纳),最近疟疾的抗疟处方大部分来自不合格来源(约 60%)。一些 LMICs(几内亚(31.8%)、马里(31.3%)、尼日利亚(20.4%)、肯尼亚(2.6%)和塞内加尔(2.7%))抗疟药物的使用率较低,尽管五岁以下儿童因疟疾发热从合格来源获得了高比例的抗疟药物处方。在 LMICs 中,居住在农村地区、母亲受教育程度较高以及父母财富较多的儿童因最近疟疾发热从合格来源服用抗疟药物的比例较高。
这项研究提请注意在 LMICs 中实施国家和地方一级预防策略的重要性,以限制抗疟药物的使用。这是因为大多数 LMICs 中五岁以下儿童因疟疾发热服用的抗疟药物处方不合格的比例高得惊人,而其他一些 LMICs 中不合格处方的比例更高。