Harvard Global Health Institute, Harvard University, Cambridge, Massachusetts, USA.
Department of Health Policy and Management, Harvard TH Chan School of Public Health, Boston, Massachusetts, USA.
BMJ Glob Health. 2020 Feb 11;5(2):e002023. doi: 10.1136/bmjgh-2019-002023. eCollection 2020.
Even with accessible and effective diagnostic tests and treatment, malaria remains a leading cause of death among children under five. Malaria case management requires prompt diagnosis and correct treatment but the degree to which this happens in low-income and middle-income countries (LMICs) remains largely unknown.
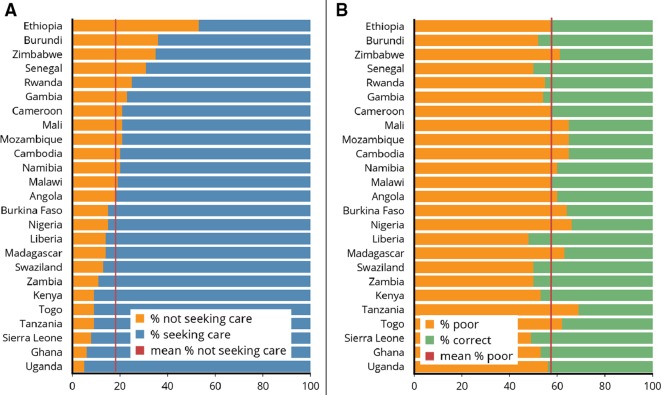
Cross-sectional study of 132 566 children under five, of which 25% reported fever in the last 2 weeks from 2006 to 2017 using the latest Malaria Indicators Survey data across 25 malaria-endemic countries. We calculated the per cent of patient encounters of febrile children under five that received poor quality of care (no blood testing, less or more than two antimalarial drugs and delayed treatment provision) across each treatment cascade and region.
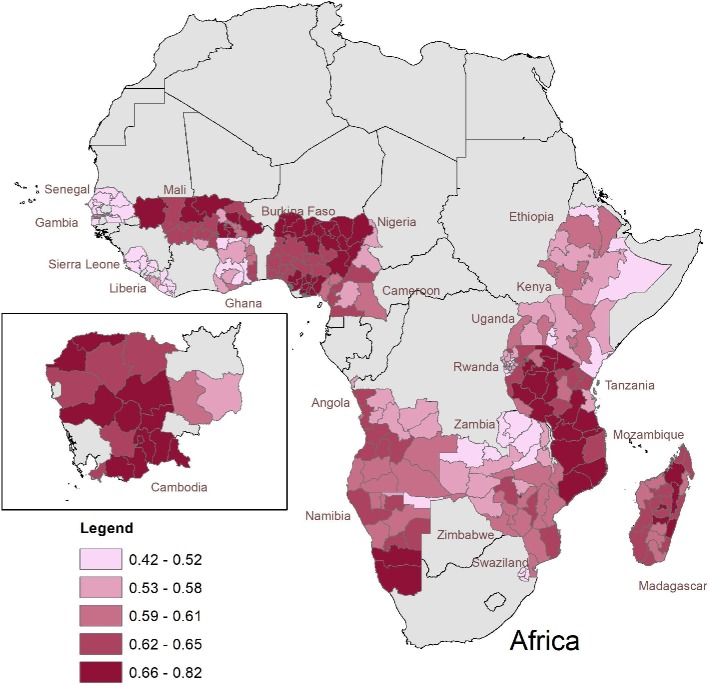
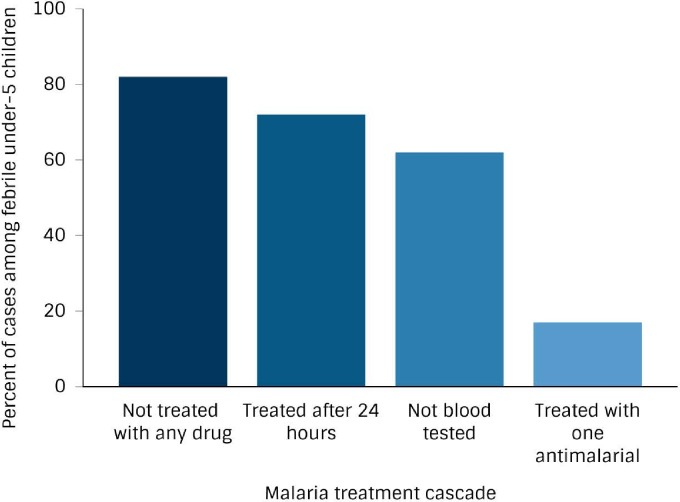
Across the study countries, 48 316 (58%) of patient encounters of febrile children under five received poor quality of care for suspected malaria. When comparing by treatment cascade, 62% of cases were not blood tested despite reporting fever in the last 2 weeks, 82% did not receive any antimalarial drug, 17% received one drug and 72% received treatment more than 24 hours after onset of fever. Of the four countries where we had more detailed malaria testing data, we found that 35% of patients were incorrectly managed (26% were undertreated, while 9% were overtreated). Poor malaria care quality varies widely within and between countries.
Quality of malaria care remains poor and varies widely in endemic LMICs. Treatments are often prescribed regardless of malaria test results, suggesting that presumptive diagnosis is still commonly practiced among cases of suspected malaria, rather than the WHO recommendation of 'test and treat'. To reach the 2030 global malaria goal of reducing mortality rates by at least 90%, focussing on improving the quality of malaria care is needed.
即使有了易于获取且有效的诊断检测和治疗方法,疟疾仍然是五岁以下儿童死亡的主要原因。疟疾病例管理需要及时诊断和正确治疗,但在低收入和中等收入国家(LMICs)中,这种情况的发生程度在很大程度上仍不得而知。
使用最新的疟疾指标调查数据,对 2006 年至 2017 年期间来自 25 个疟疾流行国家的 132566 名五岁以下儿童进行了横断面研究,其中 25%的儿童在过去 2 周内有发热报告。我们计算了在每个治疗环节和地区,发热的五岁以下儿童就诊中接受低质量护理(未进行血液检测、使用少于或多于两种抗疟药物以及延迟提供治疗)的患者比例。
在研究国家中,48316 名(58%)发热的五岁以下儿童就诊的疑似疟疾患者接受了低质量的护理。按治疗环节进行比较时,尽管有 62%的患者报告在过去 2 周内有发热,但未进行血液检测,82%的患者未使用任何抗疟药物,17%的患者使用了一种药物,72%的患者在发热后超过 24 小时才开始治疗。在我们有更详细疟疾检测数据的四个国家中,我们发现有 35%的患者治疗不当(26%的患者治疗不足,而 9%的患者治疗过度)。疟疾护理质量在各国国内和各国之间差异很大。
疟疾护理质量仍然很差,在疟疾流行的 LMICs 中差异很大。即使没有疟疾检测结果,也经常开出治疗药物,这表明在疑似疟疾病例中,仍然普遍采用推测性诊断,而不是世卫组织建议的“检测和治疗”。为了实现到 2030 年将全球疟疾死亡率降低至少 90%的全球目标,需要重点提高疟疾护理质量。