Cho Yong-Hwan, Choi Jaehyung, Huh Chae-Wook, Kim Chang Hyeun, Chang Chul Hoon, Kwon Soon Chan, Kim Young Woo, Sheen Seung Hun, Park Sukh Que, Ko Jun Kyeung, Ha Sung-Kon, Jeong Hae Woong, Kang Hyen Seung
Department of Neurosurgery, Dong-A University Hospital, Busan, Korea.
Department of Neurosurgery, Busan-Ulsan Regional Cardiocerebrovascular Center, Dong-A University Hospital, Busan, Korea.
J Cerebrovasc Endovasc Neurosurg. 2024 Mar;26(1):1-10. doi: 10.7461/jcen.2024.E2023.08.008. Epub 2024 Mar 25.
Endovascular coil embolization is the primary treatment modality for intracranial aneurysms. However, its long-term durability remains of concern, with a considerable proportion of cases requiring aneurysm reopening and retreatment. Therefore, establishing optimal follow-up imaging protocols is necessary to ensure a durable occlusion. This study aimed to develop guidelines for follow-up imaging strategies after endovascular treatment of intracranial aneurysms.
A committee comprising members of the Korean Neuroendovascular Society and other relevant societies was formed. A literature review and analyses of the major published guidelines were conducted to gather evidence. A panel of 40 experts convened to achieve a consensus on the recommendations using the modified Delphi method.
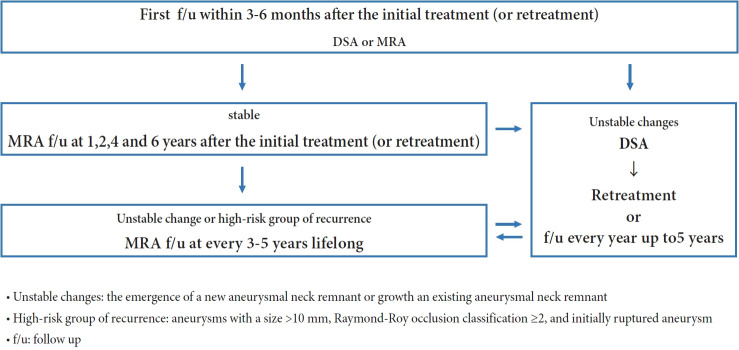
The panel members reached the following consensus: 1. Schedule the initial follow-up imaging within 3-6 months of treatment. 2. Noninvasive imaging modalities, such as three-dimensional time-of-flight magnetic resonance angiography (MRA) or contrast-enhanced MRA, are alternatives to digital subtraction angiography (DSA) during the first follow-up. 3. Schedule mid-term follow-up imaging at 1, 2, 4, and 6 years after the initial treatment. 4. If noninvasive imaging reveals unstable changes in the treated aneurysms, DSA should be considered. 5. Consider late-term follow-up imaging every 3-5 years for lifelong monitoring of patients with unstable changes or at high risk of recurrence.
The guidelines aim to provide physicians with the information to make informed decisions and provide patients with high-quality care. However, owing to a lack of specific recommendations and scientific data, these guidelines are based on expert consensus and should be considered in conjunction with individual patient characteristics and circumstances.
血管内弹簧圈栓塞术是颅内动脉瘤的主要治疗方式。然而,其长期耐久性仍令人担忧,相当一部分病例需要再次打开动脉瘤并进行再次治疗。因此,制定最佳的随访成像方案对于确保持久闭塞是必要的。本研究旨在制定颅内动脉瘤血管内治疗后随访成像策略的指南。
成立了一个由韩国神经血管内介入学会成员和其他相关学会成员组成的委员会。进行了文献综述并分析了主要已发表的指南以收集证据。召集了40位专家组成的小组,使用改良的德尔菲法就这些建议达成共识。
小组成员达成了以下共识:1. 在治疗后3 - 6个月安排首次随访成像。2. 在首次随访期间,非侵入性成像方式,如三维时间飞跃磁共振血管造影(MRA)或对比增强MRA,可作为数字减影血管造影(DSA)的替代方法。3. 在初始治疗后的1、2、4和6年安排中期随访成像。4. 如果非侵入性成像显示治疗的动脉瘤有不稳定变化,应考虑进行DSA检查。5. 对于有不稳定变化或复发高风险的患者,考虑每3 - 5年进行晚期随访成像,以进行终身监测。
这些指南旨在为医生提供信息,以便做出明智的决策,并为患者提供高质量的护理。然而,由于缺乏具体建议和科学数据依据,这些指南基于专家共识,应结合个体患者的特征和情况加以考虑。