CEMAD Digestive Disease Center, Fondazione Policlinico Universitario "A. Gemelli" IRCCS, Catholic University of Rome, 00168 Rome, Italy.
Int J Mol Sci. 2024 Mar 14;25(6):3278. doi: 10.3390/ijms25063278.
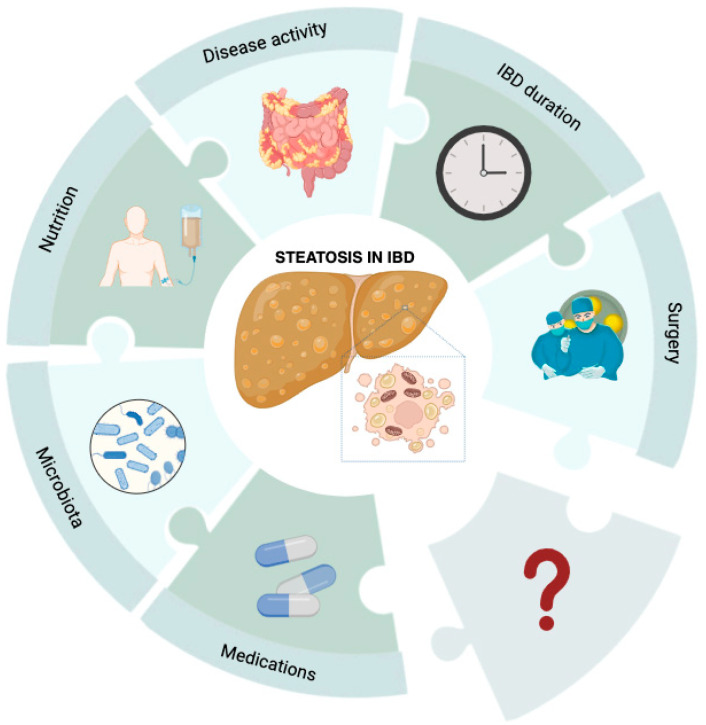
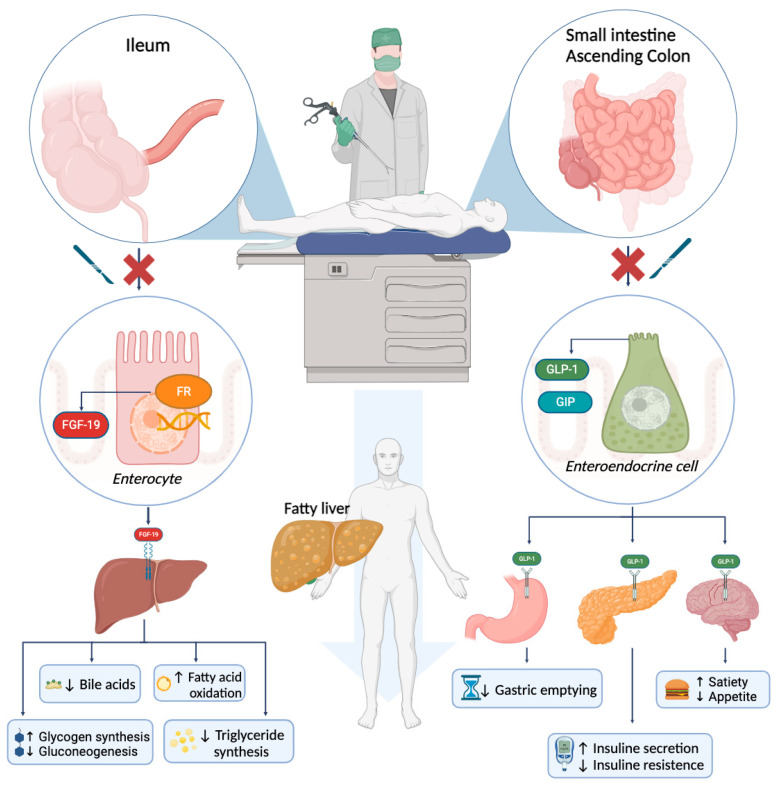
Inflammatory bowel diseases (IBD), comprising Crohn's disease and ulcerative colitis, are systemic and multifaceted disorders which affect other organs in addition to the gastrointestinal tract in up to 50% of cases. Extraintestinal manifestations may present before or after IBD diagnosis and negatively impact the intestinal disease course and patients' quality of life, often requiring additional diagnostic evaluations or specific treatments. Non-alcoholic fatty liver disease (NAFLD) is the most common liver disease worldwide. Current evidence shows an increased prevalence of NAFLD (and its more advanced stages, such as liver fibrosis and steatohepatitis) in IBD patients compared to the general population. Many different IBD-specific etiopathogenetic mechanisms have been hypothesized, including chronic inflammation, malabsorption, previous surgical interventions, changes in fecal microbiota, and drugs. However, the pathophysiological link between these two diseases is still poorly understood. In this review, we aim to provide a comprehensive overview of the potential mechanisms which have been investigated so far and highlight open issues still to be addressed for future studies.
炎症性肠病(IBD)包括克罗恩病和溃疡性结肠炎,是全身性和多方面的疾病,除了胃肠道外,在多达 50%的病例中还会影响其他器官。肠道外表现可能在 IBD 诊断之前或之后出现,并对肠道疾病的进程和患者的生活质量产生负面影响,通常需要额外的诊断评估或特定的治疗。非酒精性脂肪性肝病(NAFLD)是全球最常见的肝脏疾病。目前的证据表明,与普通人群相比,IBD 患者的 NAFLD(及其更严重的阶段,如肝纤维化和脂肪性肝炎)患病率更高。已经提出了许多不同的 IBD 特异性发病机制,包括慢性炎症、吸收不良、先前的手术干预、粪便微生物群的变化和药物。然而,这两种疾病之间的病理生理联系仍知之甚少。在这篇综述中,我们旨在全面概述迄今为止研究过的潜在机制,并强调仍需解决的未来研究的未决问题。