Conyer Ryan T, Allen Tyler G, Reinholz Anna K, Krych Aaron J, Okoroha Kelechi R, Stuart Michael J, Levy Bruce A
Department of Orthopedic Surgery, Mayo Clinic, Rochester, Minnesota, USA.
Orthop J Sports Med. 2024 Mar 26;12(3):23259671241236804. doi: 10.1177/23259671241236804. eCollection 2024 Mar.
Increased posterior tibial slope (PTS) leads to a relative anterior translation of the tibia on the femur. This is thought to decrease the stress on posterior cruciate ligament (PCL) reconstruction (PCLR) grafts.
PURPOSE/HYPOTHESIS: The purpose of this study was to analyze the effect of PTS on knee laxity, graft failure, and patient-reported outcome (PRO) scores after PCLR without concomitant anterior cruciate ligament reconstruction (ACLR). It was hypothesized that patients with higher PTS would have less knee laxity, fewer graft failures, and better PROs compared with patients with lower PTS.
Case-control study; Level of evidence, 3.
All patients who underwent PCLR between 2001 and 2020 at a single institution were identified. Patients were excluded if they underwent concomitant or prior ACLR or proximal tibial osteotomy, were younger than 18 years, had <2 years of in-person clinical follow-up, and did not have documented PRO scores (Lysholm score and International Knee Documentation Committee [IKDC] score). Data were collected retrospectively from a prospectively gathered database. PTS measurements were recorded from perioperative lateral knee radiographs. A linear regression model was created to analyze PTS in relation to PRO scores. Patients with a grade 1 (1-5 mm) or higher posterior drawer were compared with those who had a negative posterior drawer.
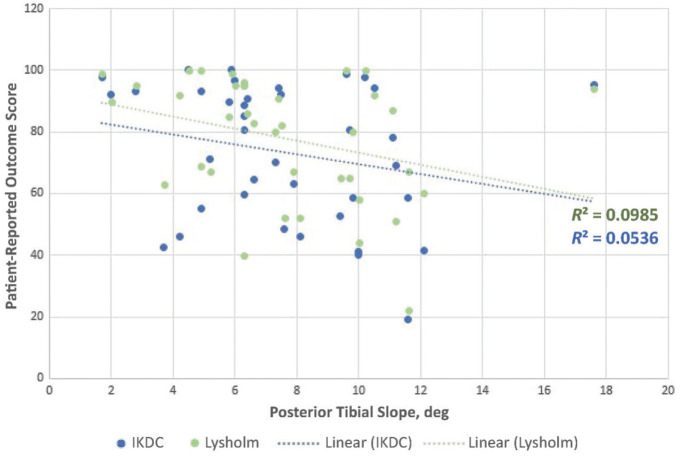
A total of 37 knees met inclusion criterion; the mean age was 30.7 years at the time of surgery. The mean clinical follow-up was 5.8 years. No significant correlation was found between either the Lysholm score or the IKDC score and the PTS. Twelve knees (32.4%) had a positive posterior drawer at final follow-up. The mean PTS in knees with a positive posterior drawer was 6.2°, whereas that for knees with a negative posterior drawer was 8.3° ( = .08). No significant differences in PRO scores were identified for knees with versus knees without a positive posterior drawer. No documented graft failures or revisions were found.
No significant differences were found in PROs or graft failure rates based on PTS at a mean of 5.8 years after PCLR. Increased tibial slope trended toward being protective against a positive posterior drawer, although this did not reach statistical significance.
胫骨后倾坡度(PTS)增加会导致胫骨在股骨上相对向前移位。这被认为可减轻后交叉韧带(PCL)重建(PCLR)移植物上的应力。
目的/假设:本研究的目的是分析PTS对单纯PCL重建(不伴前交叉韧带重建[ACLR])术后膝关节松弛度、移植物失败及患者报告结局(PRO)评分的影响。假设与PTS较低的患者相比,PTS较高的患者膝关节松弛度更小、移植物失败更少且PRO更好。
病例对照研究;证据等级:3级。
确定2001年至2020年在单一机构接受PCLR的所有患者。若患者接受过同期或既往ACLR或胫骨近端截骨术、年龄小于18岁、亲自临床随访时间不足2年且无记录的PRO评分(Lysholm评分和国际膝关节文献委员会[IKDC]评分),则将其排除。数据从前瞻性收集的数据库中进行回顾性收集。从围手术期膝关节侧位X线片记录PTS测量值。建立线性回归模型以分析PTS与PRO评分的关系。将后抽屉试验为1级(1 - 5毫米)或更高等级的患者与后抽屉试验为阴性的患者进行比较。
共有37个膝关节符合纳入标准;手术时平均年龄为30.7岁。平均临床随访时间为5.8年。未发现Lysholm评分或IKDC评分与PTS之间存在显著相关性。在末次随访时,12个膝关节(32.4%)后抽屉试验为阳性。后抽屉试验为阳性的膝关节平均PTS为6.2°,而后抽屉试验为阴性的膝关节平均PTS为8.3°(P = 0.08)。后抽屉试验为阳性的膝关节与后抽屉试验为阴性的膝关节在PRO评分上未发现显著差异。未发现有记录的移植物失败或翻修情况。
在PCLR术后平均5.8年时,基于PTS的PRO或移植物失败率未发现显著差异。胫骨坡度增加虽未达到统计学意义,但有降低后抽屉试验为阳性的趋势。