University of Florence, Department of Experimental and Clinical Medicine, Industrial Hygiene and Toxicology Laboratory, Florence, Italy.
AOU Meyer, Health and Safety Service, Florence, Italy.
Arh Hig Rada Toksikol. 2024 Mar 29;75(1):41-50. doi: 10.2478/aiht-2024-75-3803. eCollection 2024 Mar 1.
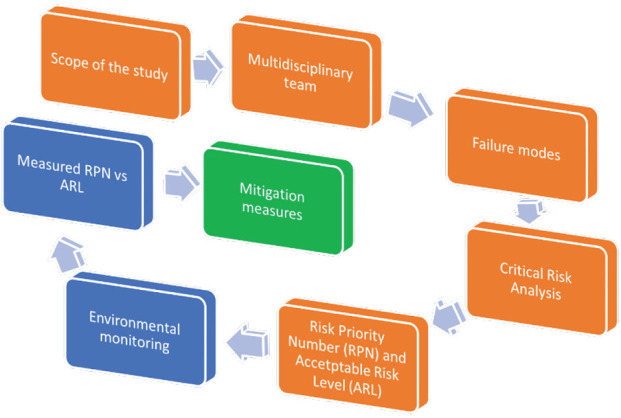
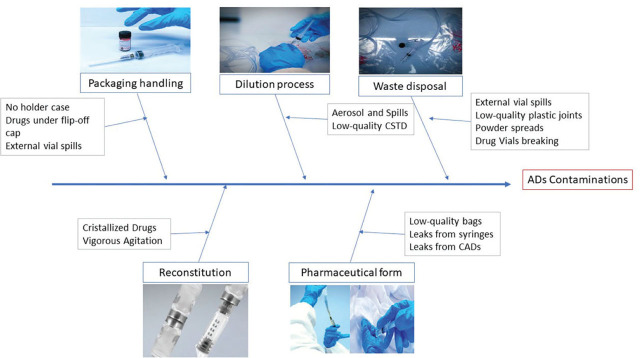
Healthcare workers handling antineoplastic drugs (ADs) in preparation units run the risk of occupational exposure to contaminated surfaces and associated mutagenic, teratogenic, and oncogenic effects of those drugs. To minimise this risk, automated compounding systems, mainly robots, have been replacing manual preparation of intravenous drugs for the last 20 years now, and their number is on the rise. To evaluate contamination risk and the quality of the working environment for healthcare workers preparing ADs, we applied the Failure Mode Effects and Criticality Analysis (FMECA) method to compare the acceptable risk level (ARL), based on the risk priority number (RPN) calculated from five identified failure modes, with the measured risk level (MRL). The model has shown higher risk of exposure with powdered ADs and containers not protected by external plastic shrink film, but we found no clear difference in contamination risk between manual and automated preparation. This approach could be useful to assess and prevent the risk of occupational exposure for healthcare workers coming from residual cytotoxic contamination both for current handling procedures and the newly designed ones. At the same time, contamination monitoring data can be used to keep track of the quality of working conditions by comparing the observed risk profiles with the proposed ARL. Our study has shown that automated preparation may have an upper hand in terms of safety but still leaves room for improvement, at least in our four hospitals.
医护人员在准备单元中处理抗肿瘤药物(AD)时,有接触受污染表面的职业风险,并且这些药物具有诱变、致畸和致癌作用。为了最大限度地降低这种风险,自动化配药系统,主要是机器人,已经在过去 20 年中取代了静脉药物的手动配制,而且其数量还在增加。为了评估医护人员准备 AD 时的污染风险和工作环境质量,我们应用失效模式影响及关键度分析(FMECA)方法,将基于五个已识别失效模式计算的风险优先数(RPN)与测量的风险水平(MRL)进行比较,来评估可接受的风险水平(ARL)。模型显示,粉状 AD 和未用外部塑料收缩膜保护的容器存在更高的暴露风险,但我们发现手动和自动化准备之间的污染风险没有明显差异。这种方法可用于评估和预防医护人员因细胞毒性残留污染而接触的职业风险,不仅适用于当前的处理程序,也适用于新设计的程序。同时,污染监测数据可用于通过将观察到的风险概况与建议的 ARL 进行比较,跟踪工作条件的质量。我们的研究表明,自动化准备在安全性方面可能具有优势,但至少在我们的四家医院中,仍有改进的空间。