Kuhle Jens, Leppert David, Comi Giancarlo, de Stefano Nicola, Kappos Ludwig, Freedman Mark S, Seitzinger Andrea, Roy Sanjeev
Department of Neurology, University Hospital Basel, Petersgraben 4, Basel CH-4031, Switzerland.
Multiple Sclerosis Centre and Research Center for Clinical Neuroimmunology and Neuroscience (RC2NB), Departments of Biomedicine and Clinical Research, University Hospital and University of Basel, Spitalstrasse 2, Basel CH-4031, Switzerland.
Ther Adv Neurol Disord. 2024 Mar 29;17:17562864241239101. doi: 10.1177/17562864241239101. eCollection 2024.
In REFLEX, subcutaneous interferon beta-1a (sc IFN β-1a) delayed the onset of multiple sclerosis (MS) in patients with a first clinical demyelinating event (FCDE).
This analysis aimed to determine whether baseline serum neurofilament light (sNfL) chain can predict conversion to MS and whether correlations exist between baseline sNfL and magnetic resonance imaging (MRI) metrics.
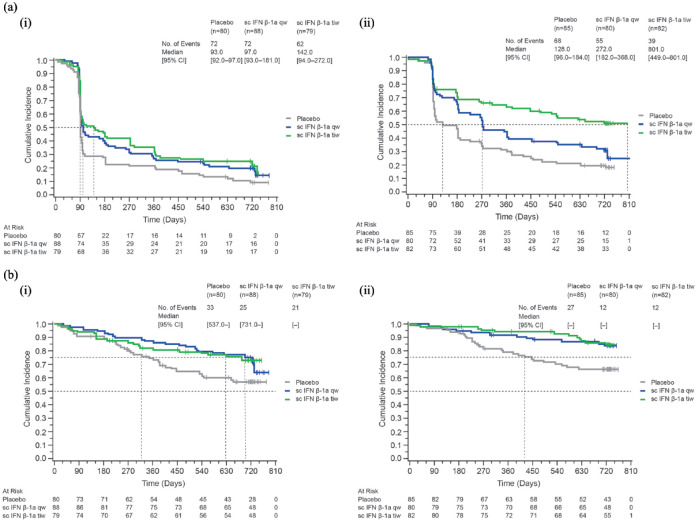
sNfL was measured for 494 patients who received sc IFN β-1a 44 μg once weekly (qw; = 168), three times weekly (tiw; = 161), or placebo ( = 165) over 24 months. Median baseline sNfL (26.1 pg/mL) was used to define high/low sNfL subgroups. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated using Cox's proportional hazard model to determine factors influencing the risk of conversion to MS. Kaplan-Meier estimates calculated median time-to-conversion to MS (McDonald 2005 criteria) or clinically definite MS (CDMS; Poser criteria). Correlations between sNfL and MRI findings were assessed using Spearman's rank correlation coefficient ().
Multivariable models indicated that high baseline sNfL was associated with the likelihood of converting to MS and inversely to time-to-conversion (HR = 1.3, 95% CI: 1.03-1.64; = 0.024). Significant additional factors affecting conversion to McDonald MS were on-study treatment (sc IFN β-1a/placebo; qw: HR = 0.59, 95% CI: 0.46-0.76; tiw: HR = 0.45, 95% CI: 0.34-0.59), classification of FCDE (monofocal/multifocal; HR = 0.69, 95% CI: 0.55-0.85), and most baseline imaging findings (T2 and T1 gadolinium-enhancing [Gd+] lesions; HR = 1.02, 95% CI: 1.01-1.03 and HR = 1.07, 95% CI: 1.03-1.11); all ⩽ 0.001. Conversion to CDMS showed similar results. At month 24, sNfL was strongly correlated with a mean number of combined unique active ( = 0.71), new T2 ( = 0.72), and new T1 Gd+ ( = 0.60) lesions; weak correlations were observed between sNfL and clinical outcomes for all treatment groups.
Higher baseline sNfL was associated with an increased risk of MS conversion, a risk that was mitigated by treatment with sc IFN β-1a tiw.
ClinicalTrials.gov identifier: NCT00404352. Date registered: 28 November 2006.
在REFLEX研究中,皮下注射干扰素β-1a(sc IFN β-1a)延缓了首次临床脱髓鞘事件(FCDE)患者多发性硬化症(MS)的发病。
本分析旨在确定基线血清神经丝轻链(sNfL)是否可预测向MS的转化,以及基线sNfL与磁共振成像(MRI)指标之间是否存在相关性。
对494例患者进行sNfL检测,这些患者在24个月内接受每周一次(qw;n = 168)、每周三次(tiw;n = 161)的44μg sc IFN β-1a治疗或安慰剂(n = 165)治疗。采用基线sNfL中位数(26.1 pg/mL)定义sNfL高/低亚组。使用Cox比例风险模型计算风险比(HR)和95%置信区间(CI),以确定影响向MS转化风险的因素。采用Kaplan-Meier估计法计算达到MS转化(McDonald 2005标准)或临床确诊MS(CDMS;Poser标准)的中位时间。使用Spearman等级相关系数(ρ)评估sNfL与MRI结果之间的相关性。
多变量模型表明,基线sNfL高与向MS转化的可能性相关,且与转化时间呈负相关(HR = 1.3,95%CI:1.03 - 1.64;ρ = 0.024)。影响向McDonald MS转化的其他显著因素包括研究期间的治疗(sc IFN β-1a/安慰剂;qw:HR = 0.59,95%CI:0.46 - 0.76;tiw:HR = 0.45,95%CI:0.34 - 0.59)、FCDE的分类(单灶性/多灶性;HR = 0.69,95%CI:0.55 - 0.85)以及大多数基线影像学表现(T2和T1钆增强[Gd+]病灶;HR = 1.02,95%CI:1.01 - 1.03和HR = 1.07,95%CI:1.03 - 1.11);所有P⩽0.001。向CDMS转化显示出类似结果。在第24个月时,sNfL与联合独特活动性病灶平均数量(ρ = 0.71)、新T2病灶(ρ = 0.72)和新T1 Gd+病灶(ρ = 0.60)密切相关;在所有治疗组中,sNfL与临床结局之间观察到弱相关性。
较高的基线sNfL与MS转化风险增加相关,tiw方案的sc IFN β-1a治疗可降低该风险。
ClinicalTrials.gov标识符:NCT00404352。注册日期:2006年11月28日。