Ozturk Mahmut, Tongut Aybala, Sterzbecher Vanessa, Desai Manan, Esmailian Gabriel, Henmi Soichiro, Spurney Christopher, Staffa Steven J, d'Udekem Yves, Yerebakan Can
Division of Cardiac Surgery, Children's National Hospital, The George Washington University School of Medicine and Health Sciences, Washington, DC, USA.
Division of Cardiology, Children's National Hospital, The George Washington University School of Medicine and Health Sciences, Washington, DC, USA.
Interdiscip Cardiovasc Thorac Surg. 2024 Mar 29;38(4). doi: 10.1093/icvts/ivae053.
To study the risk factors for mortality, moderate or more left atrioventricular valve regurgitation (LAVVR) and reoperation after the surgical repair of complete atrioventricular septal defect (cAVSD) in a single centre.
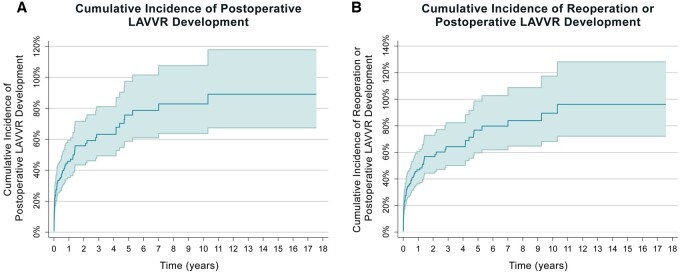
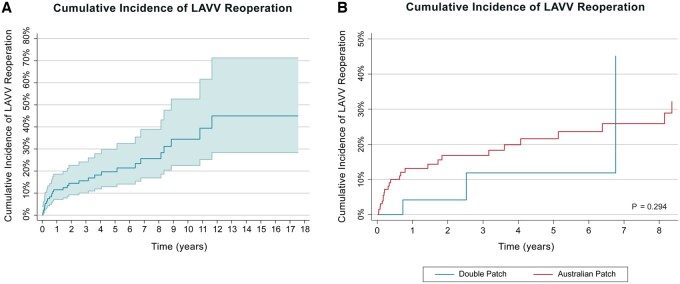
The current study is a retrospective review of patients who underwent surgical repair of cAVSD between 2000 and 2021. Patients with unbalanced ventricles not amenable to biventricular repair, double outlet right ventricle and malpositioned great arteries were excluded. The clinical predictors of outcome for end points were analysed with univariate and multivariable Cox regression analysis or Fine-Gray modelling for competing risks. Time-dependent end points were estimated using the Kaplan-Meier curve analysis and cumulative incidence curves.
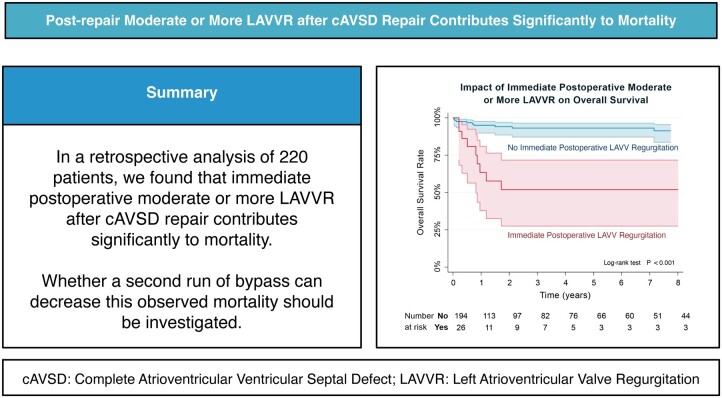
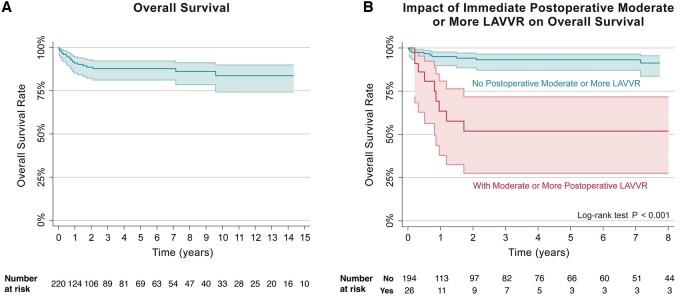
The median follow-up time was 2.3 years. Among 220 consecutive patients were 10 (4.6%) operative and 21 late mortalities (9.6%). A total of 26 patients were identified to have immediate postoperative moderate or more regurgitation and 10 of them ultimately died. By multivariable analysis prematurity and having more than moderate regurgitation immediately after the operation were identified as predictors of overall mortality (P = 0.003, P = 0.012). Five- and ten-year survival rates were lower for patients with immediate postoperative moderate or more LAVVR {51.9% [confidence interval (CI): 27.5-71.7%]} when compared to patients without moderate or more regurgitation [93.2% (CI: 87.1-96.4%) and 91.3% (CI: 83.6-95.5%)].
The patients who undergo cAVSD repair remain subjected to a heavy burden of disease related to postoperative residual LAVVR. Immediate postoperative moderate or more LAVVR contributes significantly to overall mortality. Whether a second run of bypass can decrease this observed mortality should be investigated.
在单一中心研究完全性房室间隔缺损(cAVSD)手术修复后死亡、中重度或更严重的左房室瓣反流(LAVVR)及再次手术的危险因素。
本研究是对2000年至2021年间接受cAVSD手术修复患者的回顾性分析。排除心室不平衡无法进行双心室修复、右心室双出口及大动脉位置异常的患者。采用单因素和多因素Cox回归分析或竞争风险的Fine-Gray模型分析终点结局的临床预测因素。使用Kaplan-Meier曲线分析和累积发病率曲线估计时间依赖性终点。
中位随访时间为2.3年。220例连续患者中,有10例(4.6%)术中死亡,21例(9.6%)术后晚期死亡。共26例患者术后即刻出现中重度或更严重反流,其中10例最终死亡。多因素分析显示,早产及术后即刻出现中重度以上反流是总体死亡的预测因素(P = 0.003,P = 0.012)。术后即刻出现中重度或更严重LAVVR的患者,其5年和10年生存率[51.9%(置信区间(CI):27.5 - 71.7%)]低于无中重度或更严重反流的患者[93.2%(CI:87.1 - 96.4%)和91.3%(CI:83.6 - 95.5%)]。
接受cAVSD修复的患者仍承受与术后残余LAVVR相关的沉重疾病负担。术后即刻出现中重度或更严重LAVVR对总体死亡率有显著影响。应研究再次体外循环是否能降低观察到的死亡率。