Zhang Miaomiao, Li Shuilan, Tian Chao, Li Min, Zhang Baofang, Yu Hongkui
Department of Sonography, Shenzhen Baoan Women's and Children's Hospital, Shenzhen, China.
Front Physiol. 2024 Mar 21;15:1304513. doi: 10.3389/fphys.2024.1304513. eCollection 2024.
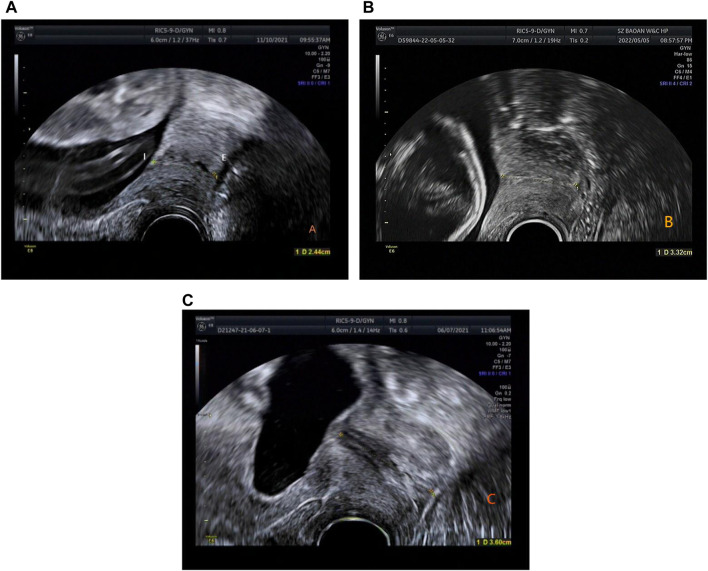
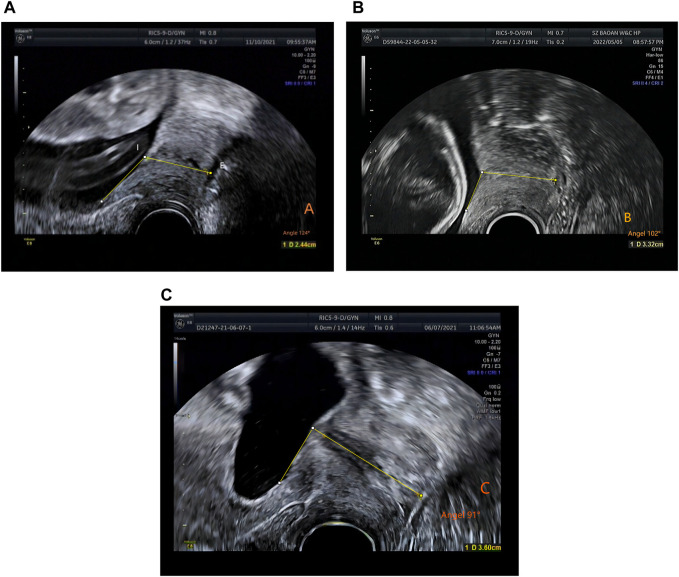
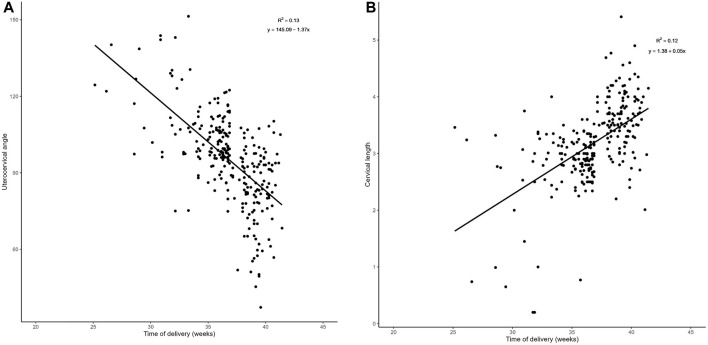
To explore the feasibility of transvaginal ultrasound measurement of uterocervical angle (UCA) and cervical length (CL) in early and mid-pregnancy and evaluate their combined prediction of spontaneous preterm birth (sPTB) in singleton pregnancies. This retrospective study comprised 274 pregnant women who underwent transvaginal ultrasound measurement of CL in mid-pregnancy (15-23+6 weeks); in 75 among them, CL also had been measured in early-pregnancy (<14 weeks). These 274 pregnant women were further divided into a preterm group (n = 149, <37 weeks gestation) and a control group (n = 125, >37 weeks gestation) according to delivery before or after 37 weeks, respectively. In the preterm group, 35 patients delivered before 34 weeks and the remaining 114 delivered between 34 and 37 weeks. The optimal threshold of CL to predict preterm birth risk in women with <37 weeks gestation was 3.38 cm, and the optimal threshold of the UCA to predict preterm birth risk in the same group of women was 96°. The optimal threshold of CL to predict preterm birth risk in women with <34 weeks gestation was 2.54 cm, while that of the UCA in the same group of patients was 106°. The area under the curve for predicting preterm birth by combining the UCA and CL measurements was greater than that by using the UCA or CL alone ( < 0.01). The sensitivity and specificity for predicting preterm birth at <34 weeks gestation was 71.7% and 86.4%, respectively; and the sensitivity and specificity for predicting preterm birth at <37 weeks gestation was 87.6% and 80.6%, respectively. The difference between the two groups in CL and UCA were not significant in early pregnancy ( > 0.01), but only in mid-pregnancy ( < 0.01). There was a negative correlation between UCA and gestational week at delivery (r = -0.361, < 0.001) and a positive correlation between CL and gestational week at delivery (r = 0.346, < 0.001) in mid-pregnancy. The proportion of deliveries at <34 weeks was highest when the UCA was >105°, and the proportion of deliveries between 35 and 37 weeks was highest when the UCA was between 95° and 105°. The proportion of deliveries at <34 weeks was highest when the CL was <2.5 cm. The combination of UCA and CL has a better ability to predict preterm birth than either measurement alone. A more obtuse UCA or a shorter CL is associated with an earlier spontaneous preterm birth. The UCA increases from early to mid-pregnancy, while the CL decreases from early to mid-pregnancy.
探讨经阴道超声测量早孕期和中孕期子宫颈角度(UCA)及宫颈长度(CL)的可行性,并评估其对单胎妊娠自发性早产(sPTB)的联合预测价值。这项回顾性研究纳入了274例在中孕期(15 - 23⁺⁶周)接受经阴道超声测量CL的孕妇;其中75例在早孕期(<14周)也测量了CL。根据分娩孕周是否在37周之前或之后,将这274例孕妇进一步分为早产组(n = 149,孕周<37周)和对照组(n = 125,孕周>37周)。在早产组中,35例患者在34周前分娩,其余114例在34至37周之间分娩。预测孕周<37周女性早产风险的CL最佳阈值为3.38 cm,同组女性预测早产风险的UCA最佳阈值为96°。预测孕周<34周女性早产风险的CL最佳阈值为2.54 cm,同组患者UCA的最佳阈值为106°。联合测量UCA和CL预测早产的曲线下面积大于单独使用UCA或CL(P<0.01)。预测孕周<34周早产的敏感性和特异性分别为71.7%和86.4%;预测孕周<37周早产的敏感性和特异性分别为87.6%和80.6%。两组在早孕期CL和UCA的差异无统计学意义(P>0.01),但仅在中孕期差异有统计学意义(P<0.01)。中孕期UCA与分娩孕周呈负相关(r = -0.361,P<0.001),CL与分娩孕周呈正相关(r = 0.346,P<0.001)。当UCA>105°时,34周前分娩的比例最高;当UCA在95°至105°之间时,35至37周分娩的比例最高。当CL<2.5 cm时,34周前分娩的比例最高。UCA和CL联合预测早产的能力优于单独测量。UCA越钝或CL越短,自发性早产越早。UCA从早孕期到中孕期增加,而CL从早孕期到中孕期减少。