NHS England, Wellington House, London, UK.
Department of Diabetes and Endocrinology, St Mary's Hospital, Imperial College Healthcare NHS Trust, London, UK.
Diabetologia. 2024 Jul;67(7):1304-1314. doi: 10.1007/s00125-024-06134-3. Epub 2024 Apr 8.
AIMS/HYPOTHESIS: The risk of dying within 2 years of presentation with diabetic foot ulceration is over six times the risk of amputation, with CVD the major contributor. Using an observational evaluation of a real-world implementation pilot, we aimed to assess whether for those presenting with diabetic foot ulceration in England, introducing a 12-lead ECG into routine care followed by appropriate clinical action was associated with reduced mortality.
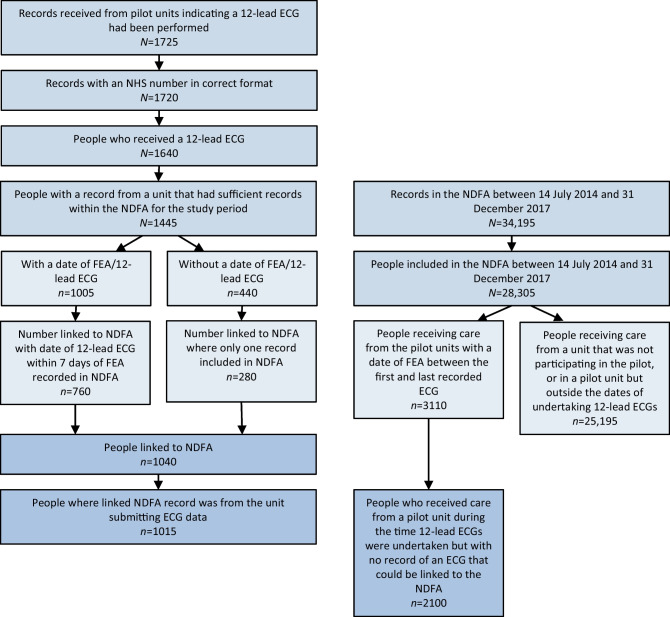
Between July 2014 and December 2017, ten multidisciplinary diabetic foot services in England participated in a pilot project introducing 12-lead ECGs for new attendees with foot ulceration. Inception coincided with launch of the National Diabetes Footcare Audit (NDFA), whereby all diabetic footcare services in England were invited to enter data on new attendees with foot ulceration. Poisson regression models assessed the mortality RR at 2 and 5 years following first assessment of those receiving care in a participating pilot unit vs those receiving care in any other unit in England, adjusting for age, sex, ethnicity, deprivation, type and duration of diabetes, ulcer severity, and morbidity in the year prior to first assessment.
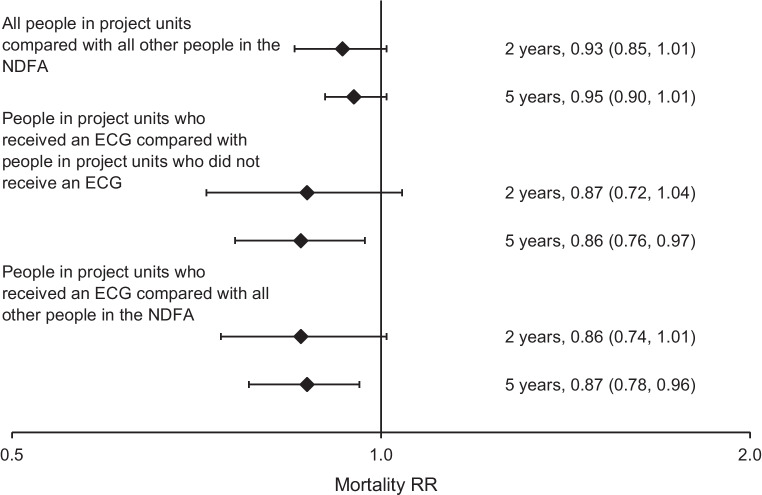
Of the 3110 people recorded in the NDFA at a participating unit during the pilot, 33% (1015) were recorded as having received an ECG. A further 25,195 people recorded in the NDFA had attended another English footcare service. Unadjusted mortality in the pilot units was 16.3% (165) at 2 years and 37.4% (380) at 5 years for those who received an ECG, and 20.5% (430) and 45.2% (950), respectively, for those who did not receive an ECG. For people included in the NDFA at other units, unadjusted mortality was 20.1% (5075) and 42.6% (10,745), respectively. In the fully adjusted model, mortality was not significantly lower for those attending participating units at 2 (RR 0.93 [95% CI 0.85, 1.01]) or 5 years (RR 0.95 [95% CI 0.90, 1.01]). At participating units, mortality in those who received an ECG vs those who did not was lower at 5 years (RR 0.86 [95% CI 0.76, 0.97]), but not at 2 years (RR 0.87 [95% CI 0.72, 1.04]). Comparing just those that received an ECG with attendees at all other centres in England, mortality was lower at 5 years (RR 0.87 [95% CI 0.78, 0.96]), but not at 2 years (RR 0.86 [95% CI 0.74, 1.01]).
CONCLUSIONS/INTERPRETATION: The evaluation confirms the high mortality seen in those presenting with diabetic foot ulceration. Overall mortality at the participating units was not significantly reduced at 2 or 5 years, with confidence intervals just crossing parity. Implementation of the 12-lead ECG into the routine care pathway proved challenging for clinical teams-overall a third of attendees had one, although some units delivered the intervention to over 60% of attendees-and the evaluation was therefore underpowered. Nonetheless, the signals of potential mortality benefit among those who had an ECG suggest that units in a position to operationalise implementation may wish to consider this.
Data from the National Diabetes Audit can be requested through the National Health Service Digital Data Access Request Service process at: https://digital.nhs.uk/services/data-access-request-service-dars/dars-products-and-services/data-set-catalogue/national-diabetes-audit-nda.
目的/假设:患有糖尿病足溃疡的患者在 2 年内死亡的风险是截肢的六倍以上,其中心血管疾病是主要因素。本研究通过对真实世界实施试点的观察性评估,旨在评估在英格兰,对于新就诊的糖尿病足溃疡患者,如果在常规护理中引入 12 导联心电图并进行适当的临床干预,是否与降低死亡率相关。
2014 年 7 月至 2017 年 12 月,英格兰的 10 个多学科糖尿病足服务机构参与了一项引入 12 导联心电图用于新就诊的足部溃疡患者的试点项目。该项目启动时恰逢英格兰国家糖尿病足部护理审计(NDFA)启动,该审计邀请英格兰所有的糖尿病足部护理服务机构上报新就诊的足部溃疡患者的数据。泊松回归模型评估了在参加试点单位接受护理的患者与在英格兰其他单位接受护理的患者,在首次评估后 2 年和 5 年的死亡率 RR,调整了年龄、性别、种族、贫困程度、糖尿病类型和持续时间、溃疡严重程度以及首次评估前一年的发病率。
在试点期间,NDFA 在参加单位记录了 3110 人,其中 33%(1015 人)被记录为接受了心电图检查。另有 25195 人在 NDFA 中记录在英格兰的其他足部护理服务就诊。在试点单位,未接受心电图检查的患者在 2 年和 5 年的死亡率分别为 16.3%(165 人)和 37.4%(380 人),而接受心电图检查的患者分别为 20.5%(430 人)和 45.2%(950 人)。在其他单位参加 NDFA 的患者中,未接受心电图检查的患者在 2 年和 5 年的死亡率分别为 20.1%(5075 人)和 42.6%(10745 人)。在完全调整的模型中,参加试点单位的患者在 2 年(RR 0.93 [95%CI 0.85,1.01])和 5 年(RR 0.95 [95%CI 0.90,1.01])的死亡率并没有显著降低。在试点单位,接受心电图检查的患者与未接受心电图检查的患者相比,5 年的死亡率较低(RR 0.86 [95%CI 0.76,0.97]),但 2 年的死亡率没有差异(RR 0.87 [95%CI 0.72,1.04])。仅比较那些接受心电图检查的患者与英格兰所有其他中心的患者,5 年的死亡率较低(RR 0.87 [95%CI 0.78,0.96]),但 2 年的死亡率没有差异(RR 0.86 [95%CI 0.74,1.01])。
结论/解释:本评估证实了患有糖尿病足溃疡的患者死亡率高。参加试点单位的患者在 2 年或 5 年的总体死亡率没有显著降低,置信区间刚刚跨越了临界点。12 导联心电图在常规护理路径中的实施对临床团队来说极具挑战性——尽管一些单位为超过 60%的患者提供了该干预措施,但总的来说只有三分之一的患者接受了心电图检查——因此评估的效能不足。尽管如此,在接受心电图检查的患者中,有潜在的死亡获益信号表明,有能力实施该方案的单位可能希望考虑这一点。
可以通过国家卫生服务数字数据访问请求服务流程在 https://digital.nhs.uk/services/data-access-request-service-dars/dars-products-and-services/data-set-catalogue/national-diabetes-audit-nda 处请求国家糖尿病审计数据。