Division of Hematology, The Ohio State University Comprehensive Cancer Center, Columbus, OH.
Weill Cornell Medicine, New York, NY.
Blood Adv. 2024 Jun 11;8(11):2861-2869. doi: 10.1182/bloodadvances.2023012142.
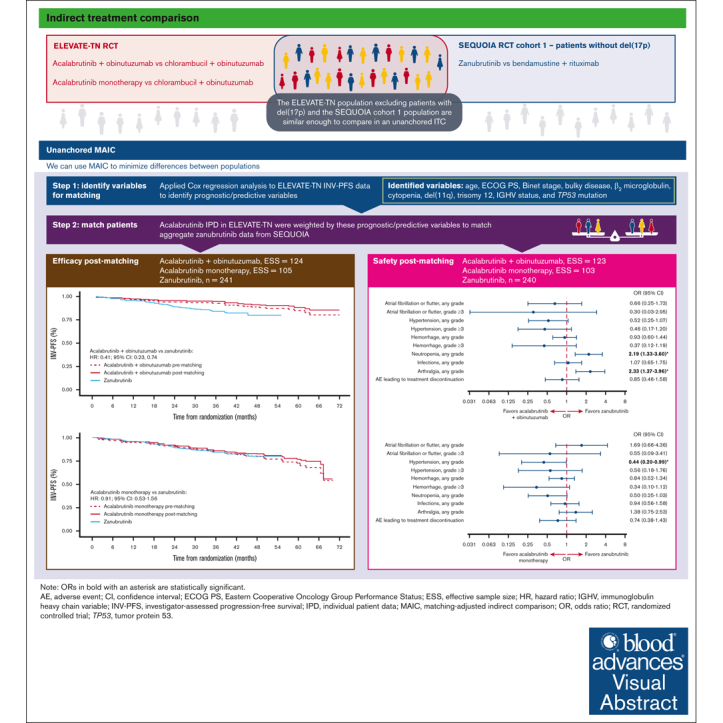
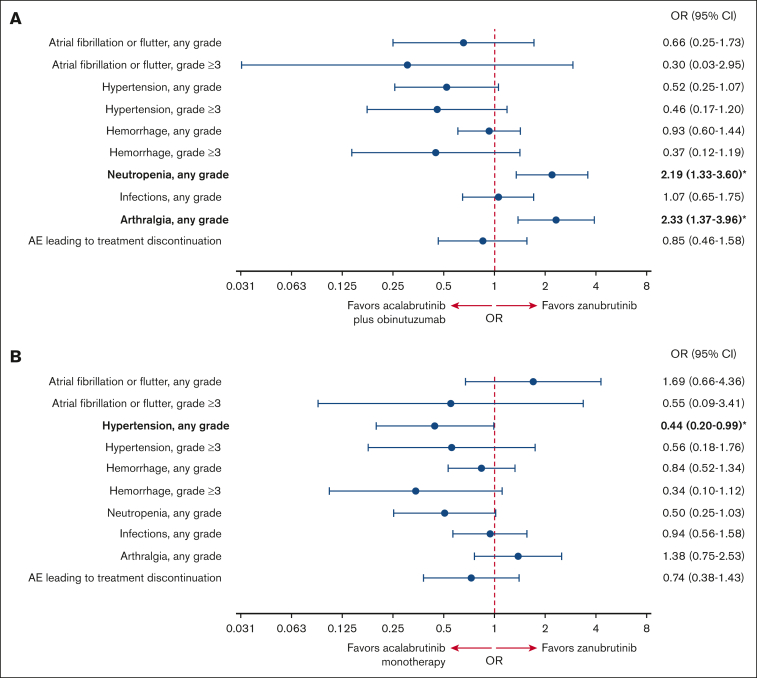
The efficacy and safety of acalabrutinib plus obinutuzumab and acalabrutinib monotherapy vs zanubrutinib in patients with treatment-naive chronic lymphocytic leukemia/small lymphocytic lymphoma without del(17p) were compared using an unanchored matching-adjusted indirect comparison. Individual patient-level data from ELEVATE-TN (acalabrutinib plus obinutuzumab, n = 162; acalabrutinib monotherapy, n = 163) were weighted to match published aggregate baseline data from SEQUOIA cohort 1, which excluded patients with del(17p) (zanubrutinib, n = 241), using variables that were prognostic/predictive of investigator-assessed progression-free survival (INV-PFS) in an exploratory Cox regression analysis of ELEVATE-TN. After matching, INV-PFS was longer with acalabrutinib plus obinutuzumab (hazard ratio [HR], 0.41; 95% confidence interval [CI], 0.23-0.74) and comparable with acalabrutinib monotherapy (HR, 0.91; 95% CI, 0.53-1.56) vs zanubrutinib. Acalabrutinib monotherapy had significantly lower odds of any grade hypertension vs zanubrutinib (odds ratio [OR], 0.44; 95% CI, 0.20-0.99), whereas acalabrutinib plus obinutuzumab had significantly higher odds of neutropenia (OR, 2.19; 95% CI, 1.33-3.60) and arthralgia (OR, 2.33; 95% CI, 1.37-3.96) vs zanubrutinib. No other significant differences in safety were observed. In summary, acalabrutinib plus obinutuzumab had longer INV-PFS with increased odds of neutropenia and arthralgia than zanubrutinib, whereas acalabrutinib monotherapy had similar INV-PFS with lower odds of any grade hypertension. These trials were registered at www.ClinicalTrials.gov as #NCT02475681 and #NCT03336333.
在未经治疗的慢性淋巴细胞白血病/小淋巴细胞淋巴瘤患者中,比较了阿卡鲁替尼联合奥滨尤妥珠单抗与阿卡鲁替尼单药治疗、泽布替尼治疗的疗效和安全性。采用无锚定匹配调整间接比较,对 ELEVATE-TN 研究(阿卡鲁替尼联合奥滨尤妥珠单抗,n=162;阿卡鲁替尼单药治疗,n=163)的个体患者水平数据进行加权,使其与 SEQUOIA 队列 1 的已发表的汇总基线数据匹配,该队列排除了 del(17p)患者(泽布替尼,n=241),使用的是探索性 Cox 回归分析 ELEVATE-TN 中预测研究者评估无进展生存期(INV-PFS)的预后/预测变量。匹配后,阿卡鲁替尼联合奥滨尤妥珠单抗的 INV-PFS 更长(风险比[HR],0.41;95%置信区间[CI],0.23-0.74),与阿卡鲁替尼单药治疗相当(HR,0.91;95%CI,0.53-1.56)vs 泽布替尼。阿卡鲁替尼单药治疗的任何级别高血压发生率明显低于泽布替尼(比值比[OR],0.44;95%CI,0.20-0.99),而阿卡鲁替尼联合奥滨尤妥珠单抗的中性粒细胞减少症(OR,2.19;95%CI,1.33-3.60)和关节痛(OR,2.33;95%CI,1.37-3.96)发生率明显高于泽布替尼。未观察到其他安全性的显著差异。总之,阿卡鲁替尼联合奥滨尤妥珠单抗的 INV-PFS 较长,中性粒细胞减少症和关节痛的发生率增加,而阿卡鲁替尼单药治疗的 INV-PFS 相似,任何级别高血压的发生率较低。这些试验在 www.ClinicalTrials.gov 上注册为 #NCT02475681 和 #NCT03336333。