Sun Yuming, Keskinocak Pinar, Steimle Lauren N, Kovacs Stephanie D, Wassilak Steven G
H. Milton Stewart School of Industrial and Systems Engineering, Georgia Institute of Technology, Atlanta, GA, USA.
Centers for Disease Control and Prevention, Atlanta, GA, USA.
Vaccine X. 2024 Mar 16;18:100476. doi: 10.1016/j.jvacx.2024.100476. eCollection 2024 Jun.
Despite the successes of the Global Polio Eradication Initiative, substantial challenges remain in eradicating the poliovirus. The Sabin-strain (live-attenuated) virus in oral poliovirus vaccine (OPV) can revert to circulating vaccine-derived poliovirus (cVDPV) in under-vaccinated communities, regain neurovirulence and transmissibility, and cause paralysis outbreaks. Since the cessation of type 2-containing OPV (OPV2) in 2016, there have been cVDPV type 2 (cVDPV2) outbreaks in four out of six geographical World Health Organization regions, making these outbreaks a significant public health threat. Preparing for and responding to cVDPV2 outbreaks requires an updated understanding of how different factors, such as outbreak responses with the novel type of OPV2 (nOPV2) and the existence of under-vaccinated areas, affect the disease spread.
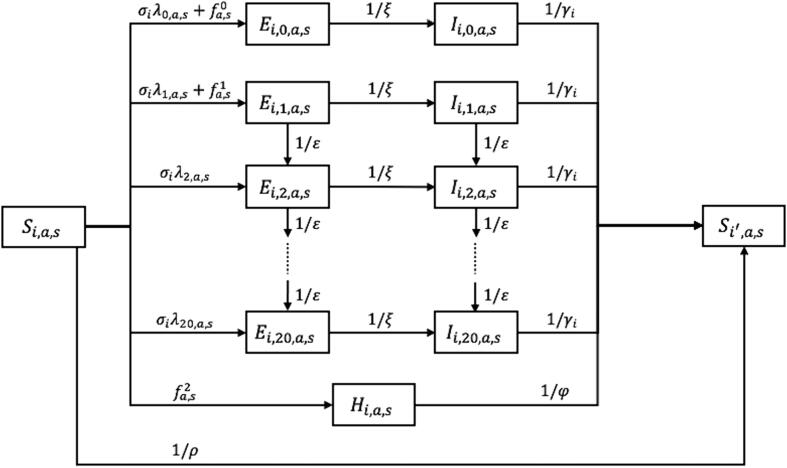
We built a differential-equation-based model to simulate the transmission of cVDPV2 following reversion of the Sabin-strain virus in prolonged circulation. The model incorporates vaccinations by essential (routine) immunization and supplementary immunization activities (SIAs), the immunity induced by different poliovirus vaccines, and the reversion process from Sabin-strain virus to cVDPV. The model's outcomes include weekly cVDPV2 paralytic case counts and the die-out date when cVDPV2 transmission stops. In a case study of Northwest and Northeast Nigeria, we fit the model to data on the weekly cVDPV2 case counts with onset in 2018-2021. We then used the model to test the impact of different outbreak response scenarios during a prediction period of 2022-2023. The response scenarios included no response, the planned response (based on Nigeria's SIA calendar), and a set of hypothetical responses that vary in the dates at which SIAs started. The planned response scenario included two rounds of SIAs that covered almost all areas of Northwest and Northeast Nigeria except some under-vaccinated areas (e.g., Sokoto). The hypothetical response scenarios involved two, three, and four rounds of SIAs that covered the whole Northwest and Northeast Nigeria. All SIAs in tested outbreak response scenarios used nOPV2. We compared the outcomes of tested outbreak response scenarios in the prediction period.
Modeled cVDPV2 weekly case counts aligned spatiotemporally with the data. The prediction results indicated that implementing the planned response reduced total case counts by 79% compared to no response, but did not stop the transmission, especially in under-vaccinated areas. Implementing the hypothetical response scenarios involving two rounds of nOPV2 SIAs that covered all areas further reduced cVDPV2 case counts in under-vaccinated areas by 91-95% compared to the planned response, with greater impact from completing the two rounds at an earlier time, but it did not stop the transmission. When the first two rounds were completed in early April 2022, implementing two additional rounds stopped the transmission in late January 2023. When the first two rounds were completed six weeks earlier (i.e., in late February 2022), implementing one (two) additional round stopped the transmission in early February 2023 (late November 2022). The die out was always achieved last in the under-vaccinated areas of Northwest and Northeast Nigeria.
A differential-equation-based model of poliovirus transmission was developed and validated in a case study of Northwest and Northeast Nigeria. The results highlighted (i) the effectiveness of nOPV2 in reducing outbreak case counts; (ii) the need for more rounds of outbreak response SIAs that covered all of Northwest and Northeast Nigeria in 2022 to stop the cVDPV2 outbreaks; (iii) that persistent transmission in under-vaccinated areas delayed the progress towards stopping outbreaks; and (iv) that a quicker outbreak response would avert more paralytic cases and require fewer SIA rounds to stop the outbreaks.
尽管全球根除脊髓灰质炎行动取得了成功,但在根除脊髓灰质炎病毒方面仍存在重大挑战。口服脊髓灰质炎疫苗(OPV)中的萨宾株(减毒活)病毒在疫苗接种不足的社区中可能会回复为循环疫苗衍生脊髓灰质炎病毒(cVDPV),恢复神经毒性和传播能力,并引发麻痹性疾病暴发。自2016年停用含2型的OPV(OPV2)以来,世界卫生组织六个地理区域中有四个出现了2型循环疫苗衍生脊髓灰质炎病毒(cVDPV2)疫情,这些疫情构成了重大的公共卫生威胁。为cVDPV2疫情做准备并应对疫情需要重新了解不同因素,如使用新型OPV2(nOPV2)的疫情应对措施以及疫苗接种不足地区的存在,如何影响疾病传播。
我们构建了一个基于微分方程的模型,以模拟萨宾株病毒在长期循环后回复为cVDPV2的传播情况。该模型纳入了基础(常规)免疫和补充免疫活动(SIAs)的疫苗接种、不同脊髓灰质炎病毒疫苗诱导的免疫以及从萨宾株病毒到cVDPV的回复过程。模型的结果包括每周cVDPV2麻痹病例数以及cVDPV2传播停止的消亡日期。在尼日利亚西北部和东北部的案例研究中,我们将模型与2018 - 2021年发病的cVDPV2每周病例数数据进行拟合。然后,我们使用该模型在2022 - 2023年的预测期内测试不同疫情应对方案的影响。应对方案包括无应对措施、计划应对措施(基于尼日利亚的SIA日程)以及一组在SIA开始日期上有所不同的假设应对措施。计划应对方案包括两轮SIA,覆盖了尼日利亚西北部和东北部几乎所有地区,但不包括一些疫苗接种不足的地区(如索科托)。假设应对方案涉及两轮、三轮和四轮覆盖整个尼日利亚西北部和东北部的SIA。测试的疫情应对方案中的所有SIA均使用nOPV2。我们比较了预测期内测试的疫情应对方案的结果。
模型模拟的cVDPV2每周病例数在时空上与数据相符。预测结果表明,与无应对措施相比,实施计划应对措施使总病例数减少了79%,但并未阻止传播,特别是在疫苗接种不足的地区。与计划应对措施相比,实施涉及两轮覆盖所有地区的nOPV2 SIA的假设应对方案,使疫苗接种不足地区的cVDPV2病例数进一步减少了91% - 95%,更早完成两轮应对措施的影响更大,但仍未阻止传播。当在2022年4月初完成前两轮时,再实施两轮可在2023年1月下旬阻止传播。当前两轮提前六周(即2022年2月下旬)完成时,再实施一轮(两轮)可在2023年2月初(2022年11月下旬)阻止传播。消亡总是在尼日利亚西北部和东北部疫苗接种不足的地区最后实现。
在尼日利亚西北部和东北部的案例研究中开发并验证了一个基于微分方程的脊髓灰质炎病毒传播模型。结果突出表明:(i)nOPV2在减少疫情病例数方面的有效性;(ii)需要在2022年进行更多轮覆盖尼日利亚西北部和东北部所有地区的疫情应对SIA,以阻止cVDPV2疫情;(iii)疫苗接种不足地区的持续传播延缓了阻止疫情的进程;(iv)更快的疫情应对将避免更多麻痹病例,并需要更少轮次的SIA来阻止疫情。



