From The Russell H. Morgan Department of Radiology and Radiological Science (P.D., L.M.F.), and Departments of Orthopaedic Surgery (L.M.F.) and Oncology (L.M.F.), The Johns Hopkins University Medical Institutions, 600 N Wolfe St, JHOC 3014, Baltimore, MD 21287; Department of Radiology (R.D.B.) and Division of Vascular Surgery, Department of Surgery (V.C.), Stanford University School of Medicine, Palo Alto, Calif; Division of Musculoskeletal Imaging and Intervention, Department of Radiology, Brigham and Women's Hospital, Harvard Medical School, Boston, Mass (S.E.S.); Infectious Disease Department, Cleveland Clinic, Cleveland, Ohio (M.B.); Department of Radiology, University of Wisconsin School of Medicine and Public Health, Madison, Wis (D.B.); Musculoskeletal Imaging and Neuroradiology, ACR Institute for Radiologic Pathology, Silver Spring, Md (M.M.); Division of Infectious Diseases and Geographic Medicine, Stanford University, Stanford, Calif (E.T.); and Department of Orthopaedic Surgery, University of California-Davis, Sacramento, Calif (C.K.).
Radiology. 2024 Apr;311(1):e231348. doi: 10.1148/radiol.231348.
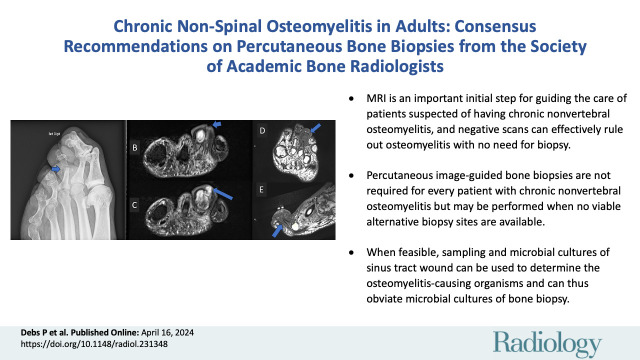
The diagnosis and management of chronic nonspinal osteomyelitis can be challenging, and guidelines regarding the appropriateness of performing percutaneous image-guided biopsies to acquire bone samples for microbiological analysis remain limited. An expert panel convened by the Society of Academic Bone Radiologists developed and endorsed consensus statements on the various indications for percutaneous image-guided biopsies to standardize care and eliminate inconsistencies across institutions. The issued statements pertain to several commonly encountered clinical presentations of chronic osteomyelitis and were supported by a literature review. For most patients, MRI can help guide management and effectively rule out osteomyelitis when performed soon after presentation. Additionally, in the appropriate clinical setting, open wounds such as sinus tracts and ulcers, as well as joint fluid aspirates, can be used for microbiological culture to determine the causative microorganism. If MRI findings are positive, surgery is not needed, and alternative sites for microbiological culture are not available, then percutaneous image-guided biopsies can be performed. The expert panel recommends that antibiotics be avoided or discontinued for an optimal period of 2 weeks prior to a biopsy whenever possible. Patients with extensive necrotic decubitus ulcers or other surgical emergencies should not undergo percutaneous image-guided biopsies but rather should be admitted for surgical debridement and intraoperative cultures. Multidisciplinary discussion and approach are crucial to ensure optimal diagnosis and care of patients diagnosed with chronic osteomyelitis.
慢性非脊柱骨髓炎的诊断和治疗具有一定挑战性,有关为进行微生物分析获取骨样本而行经皮影像引导下活检的适宜性的指南仍然有限。由骨放射学会的专家小组制定并认可了关于经皮影像引导下活检的各种适应证的共识声明,以规范治疗并消除各机构之间的差异。发布的声明涉及慢性骨髓炎的几种常见临床表现,并得到了文献复习的支持。对于大多数患者,MRI 可以帮助指导治疗,并在就诊后不久即可有效排除骨髓炎。此外,在适当的临床情况下,窦道和溃疡等开放性伤口以及关节液抽吸物可用于微生物培养以确定病原体。如果 MRI 结果阳性,则无需手术,并且无法获得其他微生物培养部位,则可以进行经皮影像引导下活检。专家小组建议,只要有可能,在活检前应尽可能避免或停用抗生素 2 周的最佳时间。广泛的坏死褥疮或其他手术急症的患者不应进行经皮影像引导下活检,而应入院进行手术清创和术中培养。多学科讨论和方法至关重要,以确保对诊断为慢性骨髓炎的患者进行最佳诊断和治疗。