University of Washington, Seattle, Washington, United States of America.
Centers for Disease Control and Prevention, Atlanta, Georgia, United States of America.
PLoS One. 2024 Apr 16;19(4):e0298628. doi: 10.1371/journal.pone.0298628. eCollection 2024.
Latent tuberculosis infection (LTBI) screening and treatment interventions that are tailored to optimize acceptance among the non-U.S.-born population are essential for U.S. tuberculosis elimination. We investigated the impact of medical interpreter use on LTBI treatment acceptance and completion among non-U.S.-born persons in a multisite study.
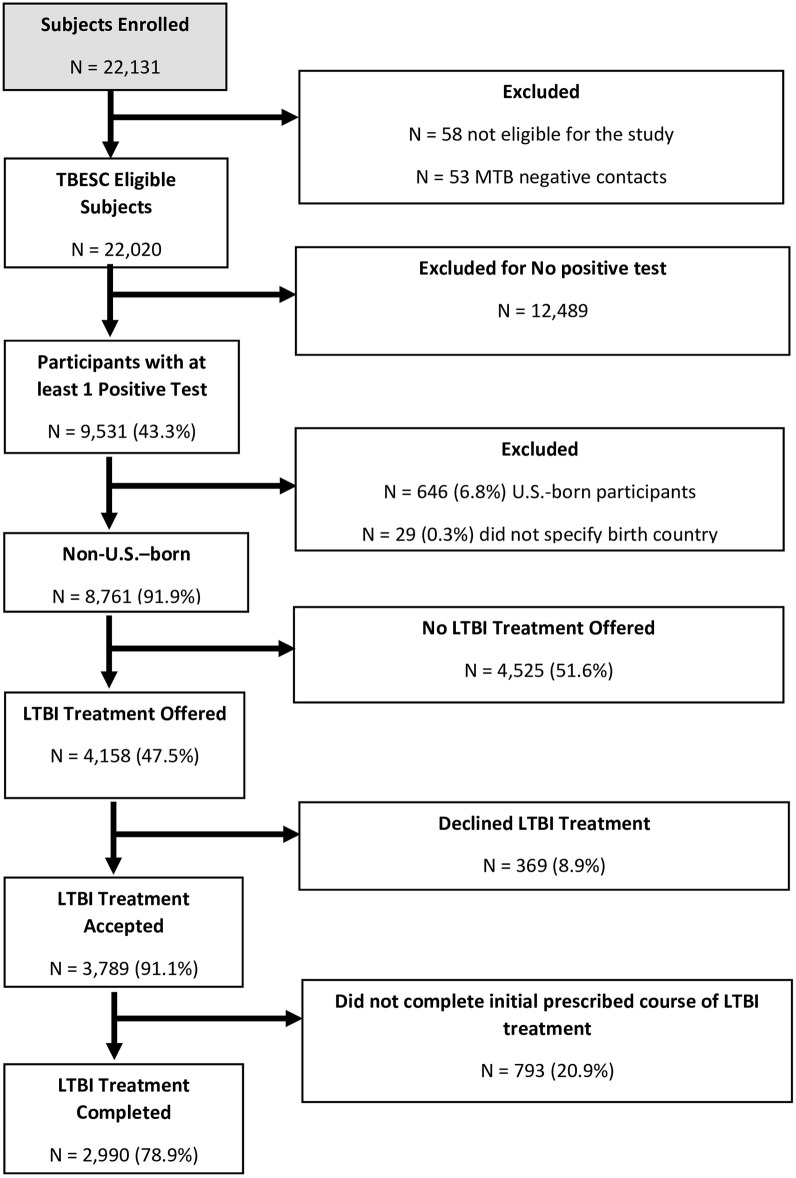
The Tuberculosis Epidemiologic Studies Consortium was a prospective cohort study that enrolled participants at high risk for LTBI at ten U.S. sites with 18 affiliated clinics from 2012 to 2017. Non-U.S.-born participants with at least one positive tuberculosis infection test result were included in analyses. Characteristics associated with LTBI treatment offer, acceptance, and completion were evaluated using multivariable logistic regression with random intercepts to account for clustering by enrollment site. Our primary outcomes were whether use of an interpreter was associated with LTBI treatment acceptance and completion. We also evaluated whether interpreter usage was associated treatment offer and whether interpreter type was associated with treatment offer, acceptance, or completion.
Among 8,761 non-U.S.-born participants, those who used an interpreter during the initial interview had a significantly greater odds of accepting LTBI treatment than those who did not use an interpreter. There was no association between use of an interpreter and a clinician's decision to offer treatment or treatment completion once accepted. Characteristics associated with lower odds of treatment being offered included experiencing homelessness and identifying as Pacific Islander persons. Lower treatment acceptance was observed in Black and Latino persons and lower treatment completion by participants experiencing homelessness. Successful treatment completion was associated with use of shorter rifamycin-based regimens. Interpreter type was not associated with LTBI treatment offer, acceptance, or completion.
We found greater LTBI treatment acceptance was associated with interpreter use among non-U.S.-born individuals.
针对非美国出生人群,优化其接受度的潜伏性结核感染(LTBI)筛查和治疗干预措施对于美国的结核病消除至关重要。我们在一项多地点研究中调查了使用医学翻译对非美国出生人群的 LTBI 治疗接受度和完成度的影响。
结核病流行病学研究联盟(Tuberculosis Epidemiologic Studies Consortium)是一项前瞻性队列研究,于 2012 年至 2017 年在美国十个地点的 18 个附属诊所招募 LTBI 高危人群。分析纳入了至少一项结核感染检测结果阳性的非美国出生参与者。使用多变量逻辑回归和随机截距,评估与 LTBI 治疗提供、接受和完成相关的特征,以解释入组地点的聚类。我们的主要结局是使用翻译是否与 LTBI 治疗接受度和完成度相关。我们还评估了翻译的使用是否与治疗提供相关,以及翻译类型是否与治疗提供、接受或完成相关。
在 8761 名非美国出生的参与者中,在初次访谈期间使用翻译的人接受 LTBI 治疗的可能性显著高于未使用翻译的人。使用翻译与临床医生提供治疗或接受治疗后完成治疗之间没有关联。与治疗提供可能性降低相关的特征包括无家可归和被认定为太平洋岛民。黑人和拉丁裔人群接受治疗的可能性较低,无家可归的参与者完成治疗的可能性较低。成功完成治疗与使用更短的利福霉素类方案相关。翻译类型与 LTBI 治疗提供、接受或完成均无关。
我们发现,在非美国出生的个体中,使用翻译与更大的 LTBI 治疗接受度相关。