Centre for Digital Health Interventions, Department of Management, Technology and Economics, ETH Zurich, Zurich, Switzerland.
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, Bern University Hospital, University of Bern, Bern, Switzerland.
JMIR Hum Factors. 2024 Apr 18;11:e46967. doi: 10.2196/46967.
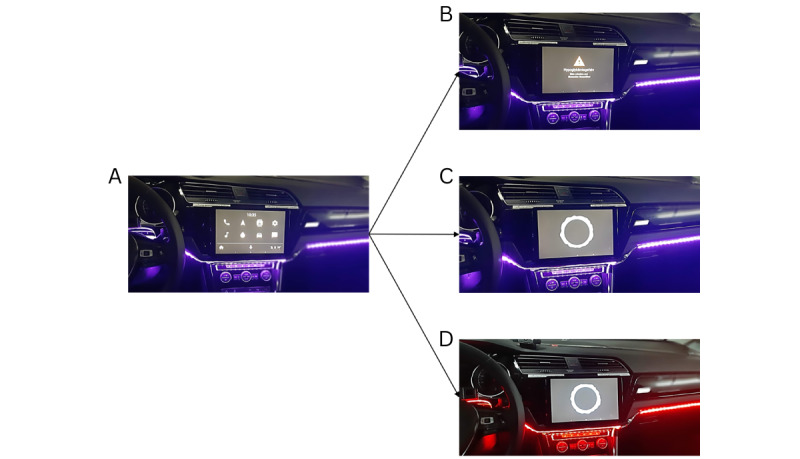
Hypoglycemia threatens cognitive function and driving safety. Previous research investigated in-vehicle voice assistants as hypoglycemia warnings. However, they could startle drivers. To address this, we combine voice warnings with ambient LEDs.
The study assesses the effect of in-vehicle multimodal warning on emotional reaction and technology acceptance among drivers with type 1 diabetes.
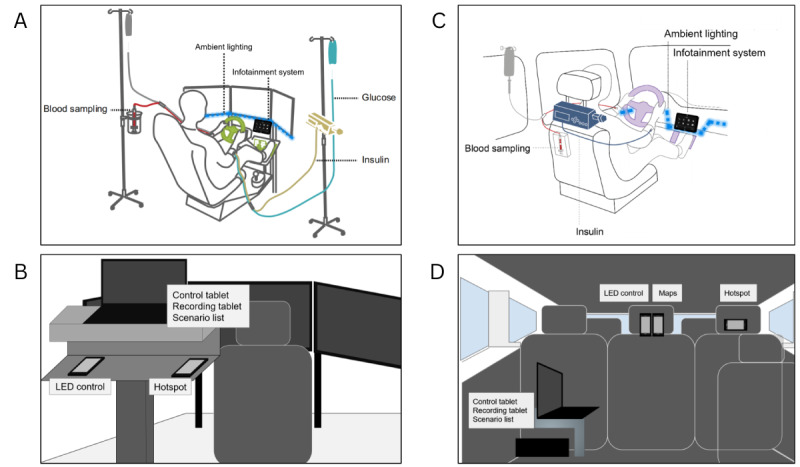
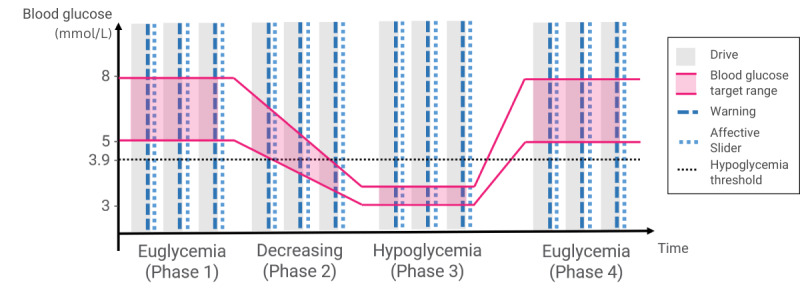
Two studies were conducted, one in simulated driving and the other in real-world driving. A quasi-experimental design included 2 independent variables (blood glucose phase and warning modality) and 1 main dependent variable (emotional reaction). Blood glucose was manipulated via intravenous catheters, and warning modality was manipulated by combining a tablet voice warning app and LEDs. Emotional reaction was measured physiologically via skin conductance response and subjectively with the Affective Slider and tested with a mixed-effect linear model. Secondary outcomes included self-reported technology acceptance. Participants were recruited from Bern University Hospital, Switzerland.
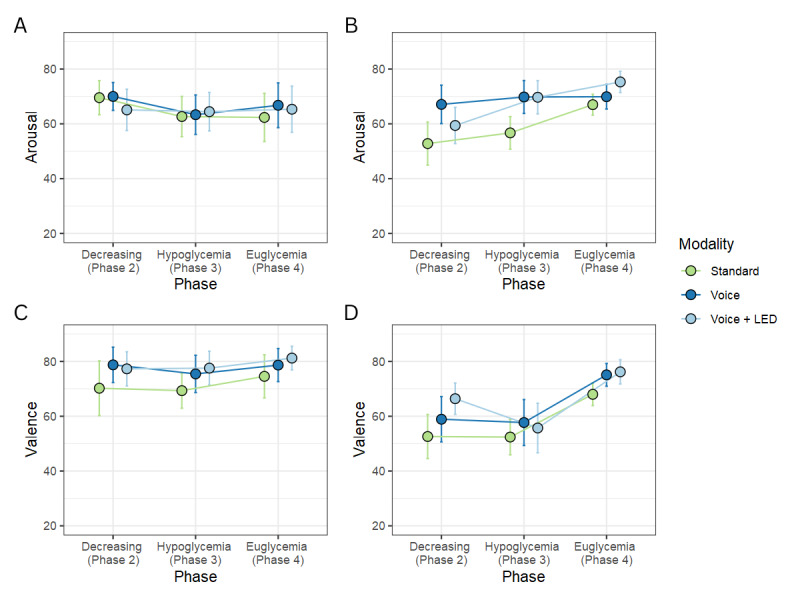
The simulated and real-world driving studies involved 9 and 10 participants with type 1 diabetes, respectively. Both studies showed significant results in self-reported emotional reactions (P<.001). In simulated driving, neither warning modality nor blood glucose phase significantly affected self-reported arousal, but in real-world driving, both did (F=4.3; P<.05 and F=4.1; P=.03). Warning modality affected self-reported valence in simulated driving (F=3.9; P<.05), while blood glucose phase affected it in real-world driving (F=9.3; P<.001). Skin conductance response did not yield significant results neither in the simulated driving study (modality: F=2.46; P=.09, blood glucose phase: F=0.3; P=.74), nor in the real-world driving study (modality: F=0.8; P=.47, blood glucose phase: F=0.7; P=.5). In both simulated and real-world driving studies, the voice+LED warning modality was the most effective (simulated: mean 3.38, SD 1.06 and real-world: mean 3.5, SD 0.71) and urgent (simulated: mean 3.12, SD 0.64 and real-world: mean 3.6, SD 0.52). Annoyance varied across settings. The standard warning modality was the least effective (simulated: mean 2.25, SD 1.16 and real-world: mean 3.3, SD 1.06) and urgent (simulated: mean 1.88, SD 1.55 and real-world: mean 2.6, SD 1.26) and the most annoying (simulated: mean 2.25, SD 1.16 and real-world: mean 1.7, SD 0.95). In terms of preference, the voice warning modality outperformed the standard warning modality. In simulated driving, the voice+LED warning modality (mean rank 1.5, SD rank 0.82) was preferred over the voice (mean rank 2.2, SD rank 0.6) and standard (mean rank 2.4, SD rank 0.81) warning modalities, while in real-world driving, the voice+LED and voice warning modalities were equally preferred (mean rank 1.8, SD rank 0.79) to the standard warning modality (mean rank 2.4, SD rank 0.84).
Despite the mixed results, this paper highlights the potential of implementing voice assistant-based health warnings in cars and advocates for multimodal alerts to enhance hypoglycemia management while driving.
ClinicalTrials.gov NCT05183191; https://classic.clinicaltrials.gov/ct2/show/NCT05183191, ClinicalTrials.gov NCT05308095; https://classic.clinicaltrials.gov/ct2/show/NCT05308095.
低血糖会威胁认知功能和驾驶安全。先前的研究调查了车载语音助手作为低血糖警告的作用。然而,它们可能会惊吓到驾驶员。为了解决这个问题,我们将语音警告与环境 LED 结合使用。
本研究评估了在 1 型糖尿病患者中,车内多模态警告对情绪反应和技术接受度的影响。
进行了两项研究,一项是模拟驾驶,另一项是实际道路驾驶。准实验设计包括 2 个独立变量(血糖阶段和警告方式)和 1 个主要因变量(情绪反应)。通过静脉导管操纵血糖,通过平板电脑语音警告应用程序和 LED 组合来操纵警告方式。使用皮肤电导率反应进行生理测量,使用情感滑块进行主观测量,并使用混合效应线性模型进行测试。次要结果包括自我报告的技术接受度。参与者是从瑞士伯尔尼大学医院招募的。
模拟和实际道路驾驶研究分别涉及 9 名和 10 名 1 型糖尿病患者。两项研究均显示在自我报告的情绪反应方面有显著结果(P<.001)。在模拟驾驶中,无论是警告方式还是血糖阶段都没有显著影响自我报告的唤醒程度,但在实际道路驾驶中,两者都有影响(F=4.3;P<.05 和 F=4.1;P=.03)。警告方式影响模拟驾驶中的自我报告效价(F=3.9;P<.05),而血糖阶段影响实际道路驾驶中的自我报告效价(F=9.3;P<.001)。皮肤电导率反应在模拟驾驶研究中没有产生显著结果(方式:F=2.46;P=.09,血糖阶段:F=0.3;P=.74),在实际道路驾驶研究中也没有产生显著结果(方式:F=0.8;P=.47,血糖阶段:F=0.7;P=.5)。在模拟驾驶和实际道路驾驶研究中,语音+LED 警告方式是最有效的(模拟:平均 3.38,SD 1.06,实际道路:平均 3.5,SD 0.71)和紧急的(模拟:平均 3.12,SD 0.64,实际道路:平均 3.6,SD 0.52)。在两种设置中,干扰程度不同。标准警告方式是最无效的(模拟:平均 2.25,SD 1.16,实际道路:平均 3.3,SD 1.06)和紧急的(模拟:平均 1.88,SD 1.55,实际道路:平均 2.6,SD 1.26)和最烦人的(模拟:平均 2.25,SD 1.16,实际道路:平均 1.7,SD 0.95)。在偏好方面,语音警告方式优于标准警告方式。在模拟驾驶中,语音+LED 警告方式(平均等级 1.5,SD 等级 0.82)优于语音(平均等级 2.2,SD 等级 0.6)和标准(平均等级 2.4,SD 等级 0.81)警告方式,而在实际道路驾驶中,语音+LED 和语音警告方式同样优先于标准警告方式(平均等级 1.8,SD 等级 0.79)。
尽管结果存在差异,但本文强调了在汽车中实施基于语音助手的健康警告的潜力,并提倡使用多模态警报来增强驾驶时的低血糖管理。
ClinicalTrials.gov NCT05183191;https://classic.clinicaltrials.gov/ct2/show/NCT05183191,ClinicalTrials.gov NCT05308095;https://classic.clinicaltrials.gov/ct2/show/NCT05308095。