UCD Centre for Precision Surgery, School of Medicine, University College Dublin, Catherine McAuley Centre, 21 Nelson St, Dublin 7, D07 KX5K, Ireland.
Department of Surgery, Mater Misericordiae University Hospital, Dublin, Ireland.
Surg Endosc. 2024 Jun;38(6):3212-3222. doi: 10.1007/s00464-024-10827-6. Epub 2024 Apr 18.
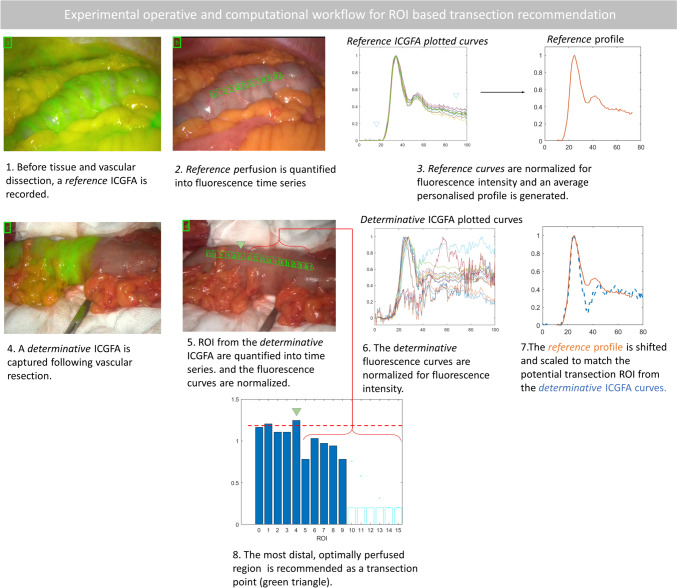
Intraoperative indocyanine green fluorescence angiography (ICGFA) aims to reduce colorectal anastomotic complications. However, signal interpretation is inconsistent and confounded by patient physiology and system behaviours. Here, we demonstrate a proof of concept of a novel clinical and computational method for patient calibrated quantitative ICGFA (QICGFA) bowel transection recommendation.
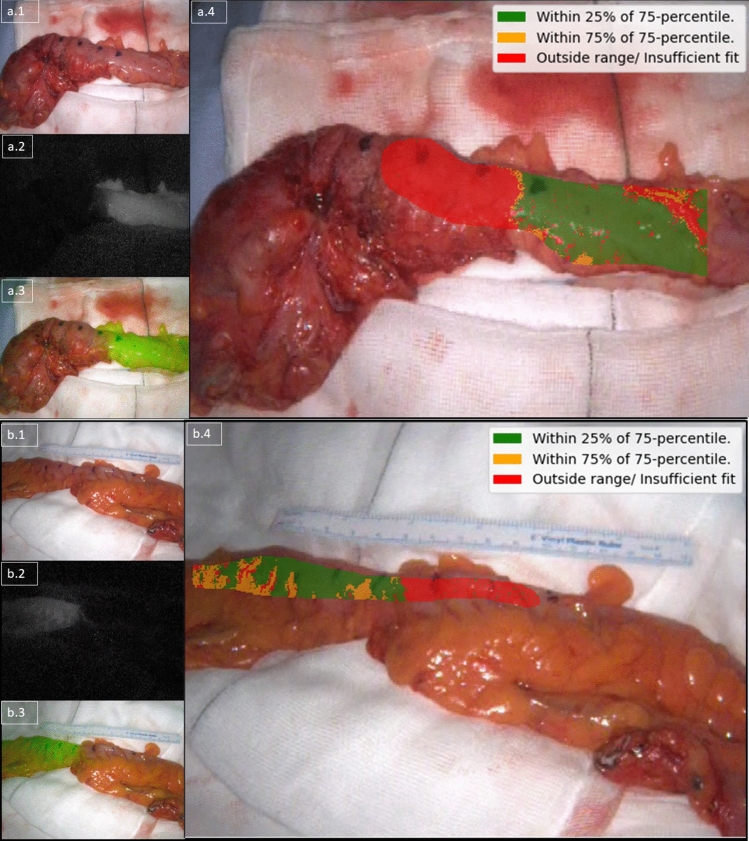
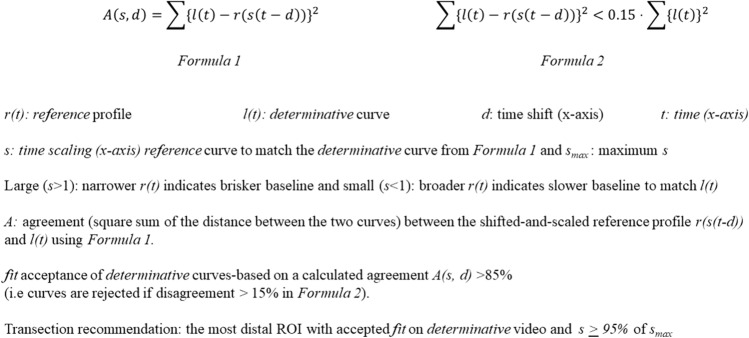
Patients undergoing elective colorectal resection had colonic ICGFA both immediately after operative commencement prior to any dissection and again, as usual, just before anastomotic construction. Video recordings of both ICGFA acquisitions were blindly quantified post hoc across selected colonic regions of interest (ROIs) using tracking-quantification software and computationally compared with satisfactory perfusion assumed in second time-point ROIs, demonstrating 85% agreement with baseline ICGFA. ROI quantification outputs detailing projected perfusion sufficiency-insufficiency zones were compared to the actual surgeon-selected transection/anastomotic construction site for left/right-sided resections, respectively. Anastomotic outcomes were recorded, and tissue lactate was also measured in the devascularised colonic segment in a subgroup of patients. The novel perfusion zone projections were developed as full-screen recommendations via overlay heatmaps.
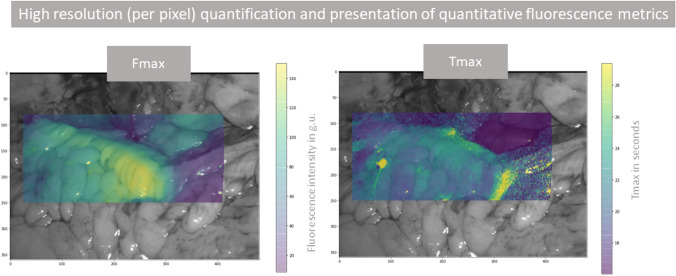
No patient suffered intra- or early postoperative anastomotic complications. Following computational development (n = 14) the software recommended zone (ROI) contained the expert surgical site of transection in almost all cases (Jaccard similarity index 0.91) of the nine patient validation series. Previously published ICGFA time-series milestone descriptors correlated moderately well, but lactate measurements did not. High resolution augmented reality heatmaps presenting recommendations from all pixels of the bowel ICGFA were generated for all cases.
By benchmarking to the patient's own baseline perfusion, this novel QICGFA method could allow the deployment of algorithmic personalised NIR bowel transection point recommendation in a way fitting existing clinical workflow.
术中吲哚菁绿荧光血管造影(ICGFA)旨在降低结直肠吻合口并发症的发生率。然而,信号解释因患者生理和系统行为而不一致和混淆。在这里,我们展示了一种新颖的临床和计算方法的概念验证,用于对患者进行校准的定量 ICGFA(QICGFA)肠横断推荐。
接受择期结直肠切除术的患者在手术开始后立即进行肠 ICGFA 检查,在进行任何解剖之前进行一次检查,然后在吻合口构建之前再次进行一次检查。使用跟踪量化软件对两次 ICGFA 采集的视频记录进行盲后定量分析,并在选定的结肠感兴趣区域(ROI)之间进行计算比较,假设第二次 ROI 的灌注是满意的,结果显示与基线 ICGFA 有 85%的一致性。ROI 量化输出详细说明了预计的灌注充足/不足区域,然后将其与实际手术医生选择的左侧/右侧切除的横断/吻合部位进行比较。记录吻合口结果,并在亚组患者中测量缺血肠段的组织乳酸。通过叠加热图,将新的灌注区域投影作为全屏推荐。
没有患者发生术中或早期术后吻合口并发症。在进行计算开发(n=14)后,该软件推荐的区域(ROI)几乎包含了 9 例患者验证系列中所有专家手术横断部位(Jaccard 相似性指数为 0.91)。以前发表的 ICGFA 时间序列里程碑描述符相关性较好,但乳酸测量相关性较差。为所有病例生成了高分辨率增强现实热图,显示了来自肠 ICGFA 所有像素的推荐。
通过与患者自身的基线灌注进行基准测试,这种新的 QICGFA 方法可以允许以适合现有临床工作流程的方式部署算法个性化近红外肠横断点推荐。