Ito Mitsuru, Yoshida Kazushi, Hidaka Azumi, Mukai Haruka, Egawa Aki
Pharmacy, The Jikei University Katsushika Medical Center, Tokyo, JPN.
Respiratory Medicine, The Jikei University Katsushika Medical Center, Tokyo, JPN.
Cureus. 2024 Mar 22;16(3):e56735. doi: 10.7759/cureus.56735. eCollection 2024 Mar.
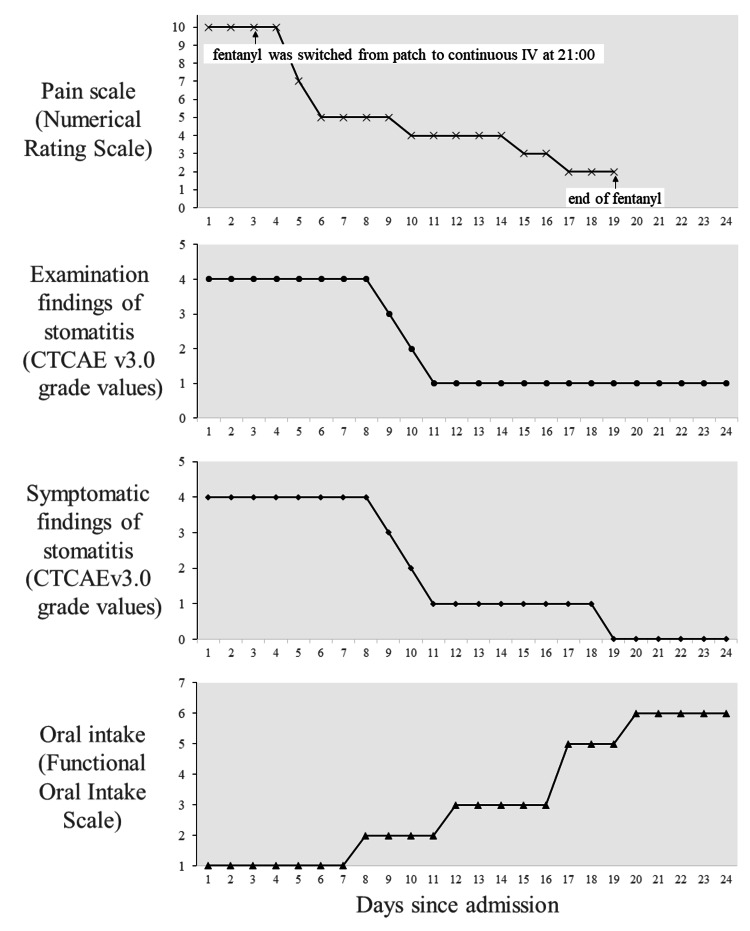
The management of oral mucosal pain in Stevens-Johnson syndrome (SJS), known for its severe mucocutaneous reactions, is a significant challenge due to the paucity of effective treatments reported in the literature. This case report aims to help fill this gap by describing the effective use of continuous intravenous fentanyl for the relief of severe oral mucosal pain in a patient with SJS. A patient with postoperative recurrence of cervical cancer developed SJS following chemotherapy. She had severe oral mucosal pain that was not relieved by 12.5 mcg/hour fentanyl transdermal patch, a regular medication. This pain was rated 10/10 on the Numerical Pain Rating Scale (NRS), and the patient had dysphagia and difficulty speaking. On admission, intravenous methylprednisolone (1000 mg/day), oral lip treatment with dexamethasone ointment, and oral rinses with azulene-lidocaine mixture were started. Analgesic treatment consisted of a 12.5 mcg/hour fentanyl transdermal patch of the regular medication and 1000 mg/dose of intravenous acetaminophen twice daily. Due to the inadequate efficacy of the transdermal patch, fentanyl was switched from the transdermal patch to a continuous intravenous fentanyl infusion at 20 mcg/hour on day three of admission. This adjustment significantly reduced pain intensity, which decreased to NRS 5/10 on day six of admission, and the patient was able to drink water and speak. Pain relief preceded clinical improvement of stomatitis. Grade 1 somnolence occurred after the start of intravenous fentanyl, but improved with follow-up. There were no other adverse effects such as respiratory depression. This case highlights the potential of intravenous fentanyl in the treatment of oral mucosal pain associated with SJS, although further studies are needed to confirm these findings and to develop comprehensive pain management protocols.
史蒂文斯-约翰逊综合征(SJS)以其严重的黏膜皮肤反应而闻名,由于文献报道的有效治疗方法匮乏,其口腔黏膜疼痛的管理面临重大挑战。本病例报告旨在通过描述连续静脉注射芬太尼在一名SJS患者中有效缓解严重口腔黏膜疼痛的情况,来填补这一空白。一名宫颈癌术后复发患者在化疗后发生了SJS。她有严重的口腔黏膜疼痛,常规用药12.5微克/小时的芬太尼透皮贴剂无法缓解。这种疼痛在数字疼痛评分量表(NRS)上评分为10分,患者有吞咽困难和说话困难。入院时,开始静脉注射甲泼尼龙(1000毫克/天),用含地塞米松软膏进行口腔唇部治疗,并用薁磺酸钠-利多卡因混合液进行口腔冲洗。镇痛治疗包括常规用药12.5微克/小时的芬太尼透皮贴剂和每日两次静脉注射对乙酰氨基酚1000毫克/剂量。由于透皮贴剂疗效不佳,在入院第三天,芬太尼从透皮贴剂改为以20微克/小时的速度连续静脉输注。这一调整显著降低了疼痛强度,在入院第六天时降至NRS 5分,患者能够喝水和说话。疼痛缓解先于口腔炎的临床改善。静脉注射芬太尼开始后出现1级嗜睡,但随访时有所改善。没有出现呼吸抑制等其他不良反应。本病例突出了静脉注射芬太尼在治疗与SJS相关的口腔黏膜疼痛方面的潜力,尽管需要进一步研究来证实这些发现并制定全面的疼痛管理方案。