Family Medicine, Mayo Clinic, Scottsdale, Arizona, USA.
Internal Medicine, Mayo Clinic, Scottsdale, Arizona, USA.
BMJ Case Rep. 2024 Apr 25;17(4):e255611. doi: 10.1136/bcr-2023-255611.
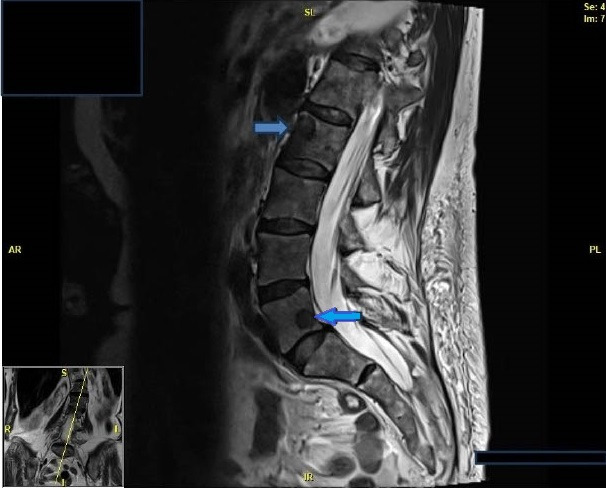
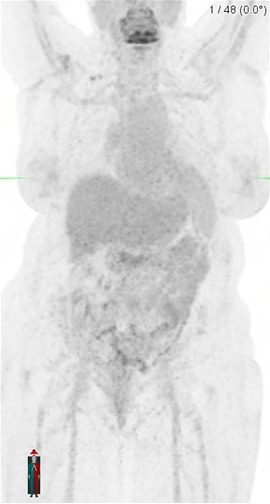
We describe a patient who had failed renal transplant after 13 years, eventually requiring a graft nephrectomy and discontinuation of immunosuppressive therapy, including antithymocyte globulin, tacrolimus and mycophenolate while on steroid avoidance protocol. Within a few months of complete discontinuation of the immunosuppressive medications, she developed lower back pain associated with numbness in her right anterolateral thigh. The radiological imaging demonstrated multiple bony lesions throughout her axial and appendicular skeleton with normal pulmonary findings. A computerised tomography-guided bone biopsy from the left iliac crest revealed fragments of bone with granulomatous inflammation, thus making the diagnosis of extrapulmonary sarcoidosis. Initiating treatment with prednisone resulted in near-complete resolution of symptoms. Long-term immunosuppressive therapy is administered to all renal transplant recipients to help prevent acute rejection and loss of renal allograft. This case highlights that immunosuppressants can conceal the presence of underlying conditions in transplant patients.
我们描述了一位患者,他在接受肾移植 13 年后移植肾失功,最终需要进行移植肾切除术,并停用包括抗胸腺细胞球蛋白、他克莫司和霉酚酸酯在内的免疫抑制剂,同时遵循激素避免方案。在完全停用免疫抑制剂药物后的几个月内,她出现了腰痛,并伴有右大腿前外侧麻木。影像学检查显示她的轴骨和附肢骨骼有多处骨病变,肺部正常。左髂嵴处的计算机断层扫描引导下的骨活检显示有肉芽肿性炎症的骨碎片,从而确诊为肺外结节病。开始使用泼尼松治疗后,症状几乎完全缓解。长期给予所有肾移植受者免疫抑制剂治疗,以帮助预防急性排斥反应和移植肾丢失。本例强调了免疫抑制剂可能会掩盖移植患者潜在疾病的存在。