Division of Digestive and Liver Diseases, Department of Internal Medicine, University of Texas Southwestern Medical Center, Dallas.
Department of Data Science, Dana-Farber Cancer Institute, Boston, Massachusetts.
JAMA Netw Open. 2024 Apr 1;7(4):e248755. doi: 10.1001/jamanetworkopen.2024.8755.
Cohort studies demonstrating an association of hepatocellular carcinoma (HCC) screening with reduced mortality are prone to lead-time and length-time biases.
To characterize the clinical benefits of HCC screening, adjusting for lead-time and length-time biases, in a diverse, contemporary cohort of at-risk patients.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study of patients with HCC was conducted between January 2008 and December 2022 at 2 large US health systems. Data analysis was performed from September to November 2023.
The primary outcome was screen-detected HCC, defined by abnormal screening-intent abdominal imaging or α-fetoprotein level within 6 months before diagnosis. Cox regression analysis was used to characterize differences in overall survival between patients with screen-detected and non-screen-detected HCC; lead-time and length-time adjustments were calculated using the Duffy parametric formula.
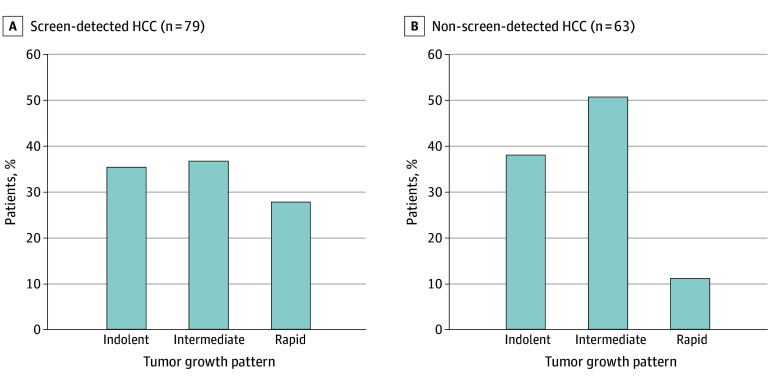
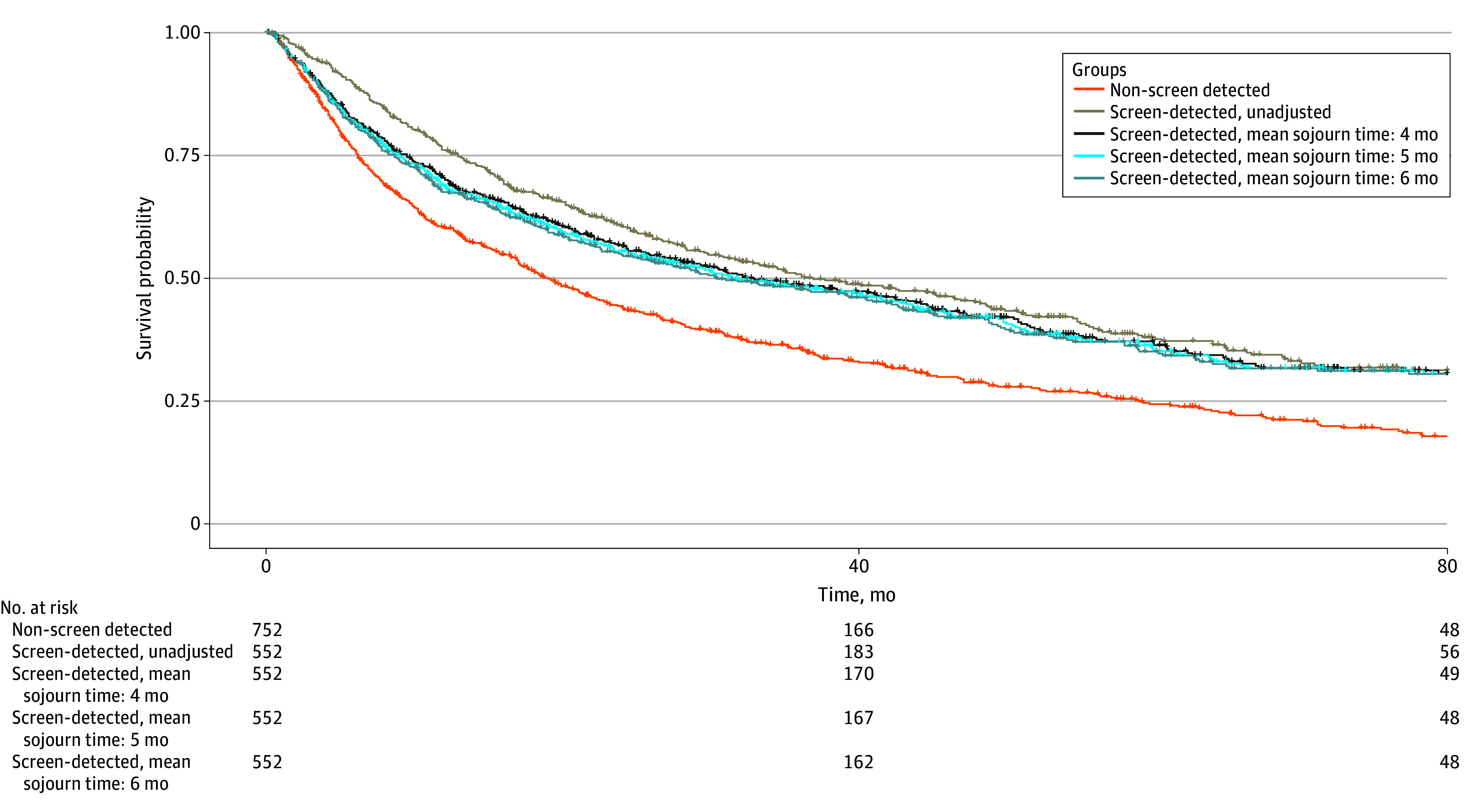
Among 1313 patients with HCC (mean [SD] age, 61.7 [9.6] years; 993 male [75.6%]; 739 [56.3%] with Barcelona Clinic Liver Cancer stage 0/A disease), HCC was screen-detected in 556 (42.3%) and non-screen detected in 757 (57.7%). Patients with screen-detected HCC had higher proportions of early-stage HCC (393 patients [70.7%] vs 346 patients [45.7%]; risk ratio [RR], 1.54; 95% CI, 1.41-1.70) and curative treatment receipt (283 patients [51.1%] vs 252 patients [33.5%]; RR, 1.52; 95% CI, 1.34-1.74) compared with patients with non-screen-detected HCC. The screen-detected group had significantly lower mortality, which persisted after correcting for lead-time bias (hazard ratio, 0.75; 95% CI, 0.65-0.87) in fully adjusted models. Both groups had similar tumor doubling times (median [IQR], 3.8 [2.2-10.7] vs 5.6 [1.7-11.4] months) and proportions of indolent tumors (28 patients [35.4%] vs 24 patients [38.1%]; RR, 0.93; 95% CI, 0.60-1.43). Adjustment for length-time bias decreased survival estimates, although 3-year and 5-year survival for patients with screen-detected HCC remained longer than that for patients with non-screen-detected HCC.
The findings of this cohort study suggest that HCC screening is associated with reduced mortality even after accounting for lead-time and length-time biases. However, these biases should be considered in future studies.
展示肝癌 (HCC) 筛查与死亡率降低相关的队列研究容易受到领先时间和持续时间偏倚的影响。
在具有风险的当代患者的多样化队列中,通过调整领先时间和持续时间偏倚来描述 HCC 筛查的临床获益。
设计、地点和参与者:这是一项在美国两个大型医疗系统中进行的 HCC 患者回顾性队列研究,于 2008 年 1 月至 2022 年 12 月进行。数据分析于 2023 年 9 月至 11 月进行。
主要结局是通过在诊断前 6 个月内进行异常筛查意向性腹部影像学检查或 α-胎蛋白水平检测发现的 HCC。使用 Cox 回归分析比较了具有筛查检测和未筛查检测 HCC 的患者之间的总体生存差异;使用 Duffy 参数公式计算了领先时间和持续时间调整。
在 1313 名 HCC 患者中(平均[SD]年龄,61.7[9.6]岁;993 名男性[75.6%];739 名[56.3%]巴塞罗那临床肝癌分期 0/A 期疾病),556 名(42.3%)为筛查检测阳性,757 名(57.7%)为筛查检测阴性。筛查检测阳性的 HCC 患者具有更高比例的早期 HCC(393 名患者[70.7%] vs 346 名患者[45.7%];风险比[RR],1.54;95%置信区间[CI],1.41-1.70)和接受根治性治疗(283 名患者[51.1%] vs 252 名患者[33.5%];RR,1.52;95% CI,1.34-1.74)与筛查检测阴性的 HCC 患者相比。在完全调整模型中,即使校正了领先时间偏倚,筛查检测组的死亡率也显著降低(风险比,0.75;95% CI,0.65-0.87)。两组的肿瘤倍增时间中位数(IQR)相似(3.8[2.2-10.7] vs 5.6[1.7-11.4]个月),惰性肿瘤的比例相似(28 名患者[35.4%] vs 24 名患者[38.1%];RR,0.93;95% CI,0.60-1.43)。尽管筛查检测 HCC 的患者 3 年和 5 年生存率仍高于未筛查检测 HCC 的患者,但对持续时间偏倚的调整降低了生存率估计。
这项队列研究的结果表明,即使考虑了领先时间和持续时间偏倚,肝癌筛查仍与死亡率降低相关。然而,未来的研究应考虑这些偏差。