Department of Cardiovascular Surgery, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, China.
Department of Cardiovascular Surgery, The First Affiliated Hospital of Zhengzhou University, Henan Province, 450052, China.
Eur J Med Res. 2024 Apr 30;29(1):260. doi: 10.1186/s40001-024-01850-3.
The objective of this study was to investigate the correlation between neutrophil-to-lymphocyte ratios (NLR) and the risk of in-hospital death in patients admitted to the intensive care unit (ICU) with both chronic kidney disease (CKD) and coronary artery disease (CAD).
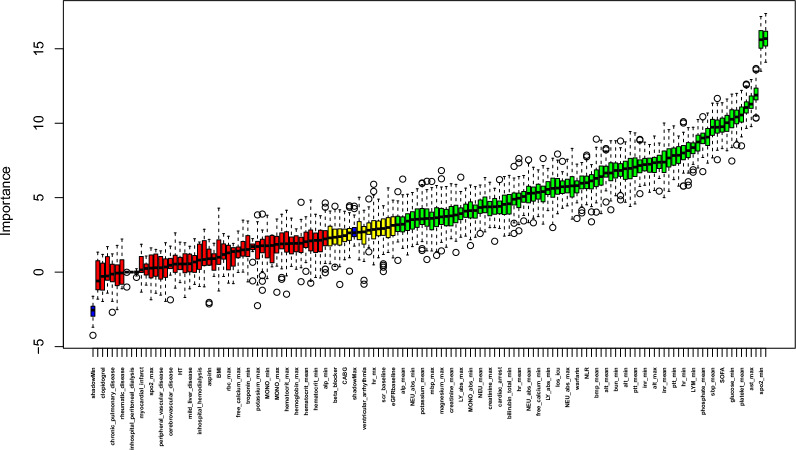
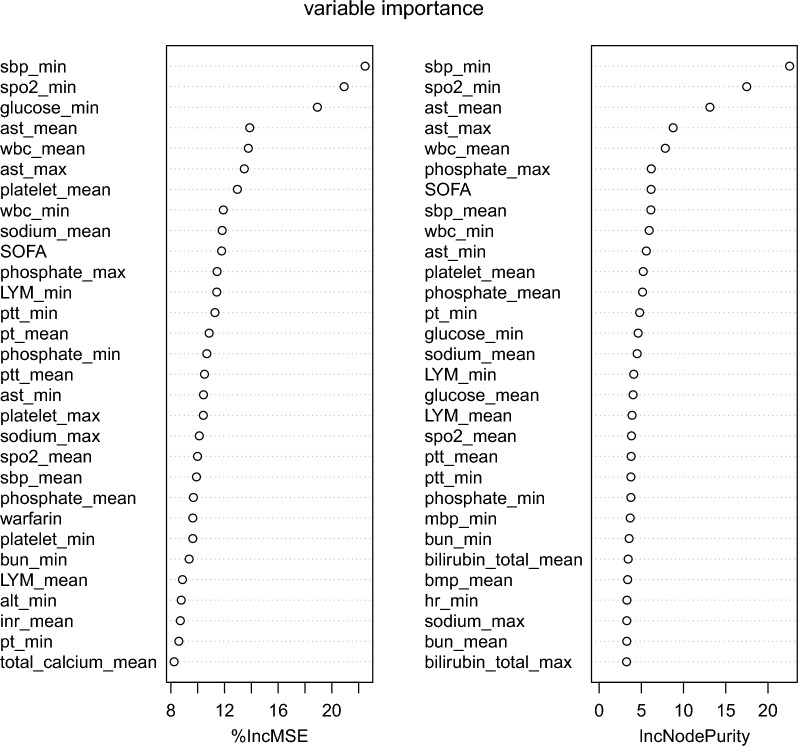
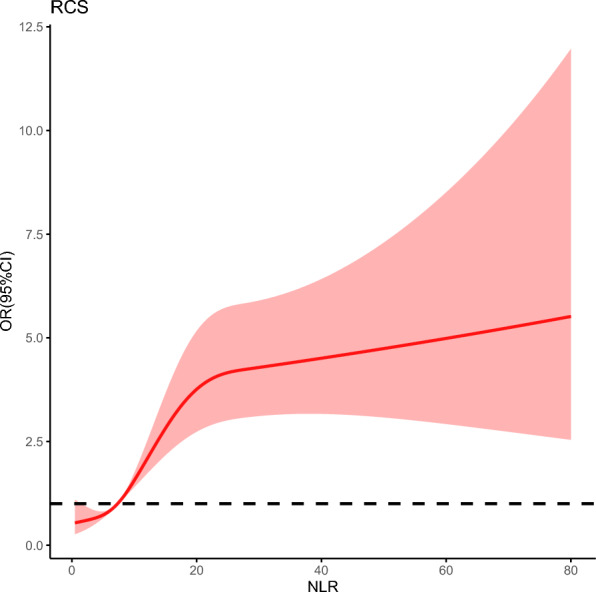
Data from the MIMIC-IV database, which includes a vast collection of more than 50,000 ICU admissions occurring between 2008 and 2019, was utilized in the study and eICU-CRD was conducted for external verification. The Boruta algorithm was employed for feature selection. Univariable and multivariable logistic regression analyses and multivariate restricted cubic spline regression were employed to scrutinize the association between NLR and in-hospital mortality. The receiver operating characteristic (ROC) curves were conducted to estimate the predictive ability of NLR.
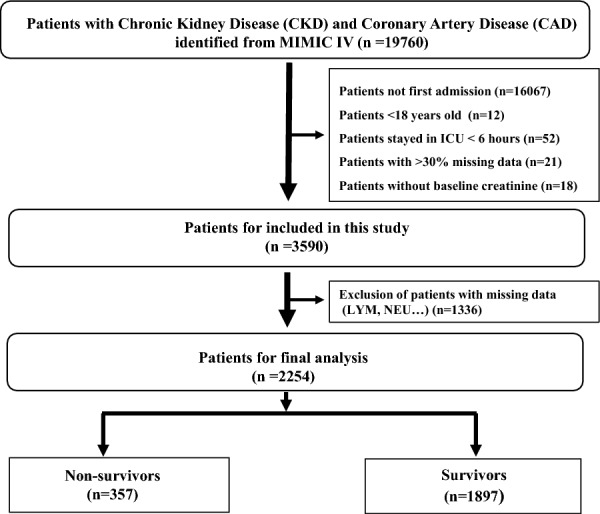
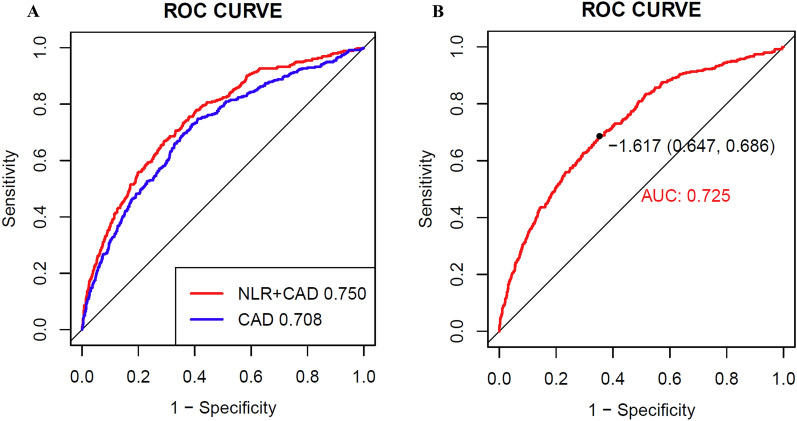
After carefully applying criteria to include and exclude participants, a total of 2254 patients with CKD and CAD were included in the research. The findings showed a median NLR of 7.3 (4.4, 12.1). The outcomes of multivariable logistic regression demonstrated that NLR significantly elevated the risk of in-hospital mortality (OR 2.122, 95% confidence interval [CI] 1.542-2.921, P < 0.001) after accounting for all relevant factors. Further insights from subgroup analyses unveiled that age and Sequential Organ Failure Assessment (SOFA) scores displayed an interactive effect in the correlation between NLR and in-hospital deaths. The NLR combined with traditional cardiovascular risk factors showed relatively great predictive value for in-hospital mortality (AUC 0.750).
The findings of this research indicate that the NLR can be used as an indicator for predicting the likelihood of death during a patient's stay in the intensive care unit, particularly for individuals with both CAD and CKD. The results indicate that NLR may serve as a valuable tool for assessing and managing risks in this group at high risk. Further investigation is required to authenticate these findings and investigate the mechanisms that underlie the correlation between NLR and mortality in individuals with CAD and CKD.
本研究旨在探讨中性粒细胞与淋巴细胞比值(NLR)与同时患有慢性肾脏病(CKD)和冠状动脉疾病(CAD)的重症监护病房(ICU)患者住院死亡风险之间的相关性。
本研究利用 MIMIC-IV 数据库的数据,该数据库包含了 2008 年至 2019 年间超过 50000 例 ICU 入院病例,并进行了 eICU-CRD 外部验证。采用 Boruta 算法进行特征选择。采用单变量和多变量逻辑回归分析以及多变量限制立方样条回归分析来探讨 NLR 与住院死亡率之间的关系。采用受试者工作特征(ROC)曲线评估 NLR 的预测能力。
经过仔细的纳入和排除标准筛选,共有 2254 例 CKD 和 CAD 患者纳入本研究。结果显示,NLR 的中位数为 7.3(4.4,12.1)。多变量逻辑回归结果表明,在考虑所有相关因素后,NLR 显著增加了住院死亡率的风险(OR 2.122,95%置信区间[CI]1.542-2.921,P<0.001)。进一步的亚组分析表明,年龄和序贯器官衰竭评估(SOFA)评分在 NLR 与住院死亡之间存在交互作用。NLR 与传统心血管危险因素联合具有较高的预测住院死亡率的价值(AUC 0.750)。
本研究结果表明,NLR 可作为预测 CAD 和 CKD 患者 ICU 住院期间死亡可能性的指标。结果表明,NLR 可能是评估和管理高危人群风险的有用工具。需要进一步的研究来验证这些发现,并探讨 NLR 与 CAD 和 CKD 患者死亡率之间相关性的机制。