Emerson Philip, Flabouris Arthas, Thomas Josephine, Fernando Jeremy, Senthuran Siva, Knowles Serena, Hammond Naomi, Sundararajan Krish
Department of Intensive Care Medicine, Royal Adelaide Hospital, Adelaide, 5000, South Australia, Australia.
University of Adelaide, 259 North Terrace, Adelaide, 5000, South Australia, Australia.
Crit Care Resusc. 2023 Dec 14;26(1):1-7. doi: 10.1016/j.ccrj.2023.10.010. eCollection 2024 Mar.
We aimed to describe the characteristics, outcomes and resource utilisation of patients being cared for in an ICU after undergoing elective surgery in Australia and New Zealand (ANZ).
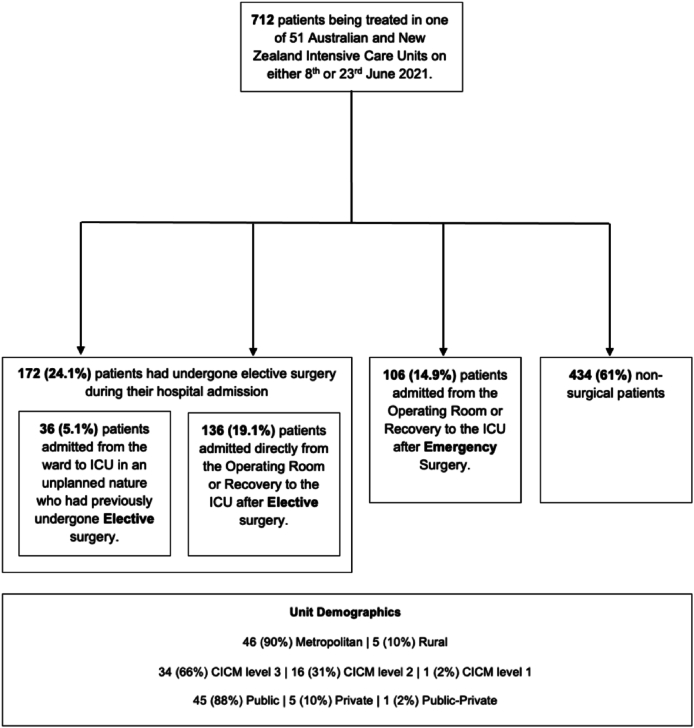
This was a point prevalence study involving 51 adult ICUs in ANZ in June 2021. Patients met inclusion criteria if they were being treated in a participating ICU on he study dates. Patients were categorised according to whether they had undergone elective surgery, admitted directly from theatre or unplanned from the ward. Descriptive and comparative analysis was performed according to the source of ICU admission. Resource utilisation was measured by Length of stay, organ support and occupied bed days.
712 patients met inclusion criteria, with 172 (24%) have undergone elective surgery. Of these, 136 (19%) were admitted directly to the ICU and 36 (5.1%) were an unplanned admission from the ward. Elective surgical patients occupied 15.8% of the total ICU patient bed days, of which 44.3% were following unplanned admissions. Elective surgical patients who were an unplanned admission from the ward, compared to those admitted directly from theatre, had a higher severity of illness (AP2 17 vs 13, p<0.01), require respiratory or vasopressor support (75% vs 44%, p<0.01) and hospital mortality (16.7% vs 2.2%, p < 0.01).
ICU resource utilisation of patients who have undergone elective surgery is substantial. Those patients admitted directly from theatre have good outcomes and low resource utilisation. Patient admitted unplanned from the ward, although fewer, were sicker, more resource intensive and had significantly worse outcomes.
我们旨在描述在澳大利亚和新西兰(ANZ)接受择期手术后在重症监护病房(ICU)接受护理的患者的特征、结局和资源利用情况。
这是一项现况研究,于2021年6月对ANZ的51个成人ICU进行。如果患者在研究日期在参与研究的ICU接受治疗,则符合纳入标准。患者根据是否接受了择期手术、直接从手术室入院或从病房非计划入院进行分类。根据ICU入院来源进行描述性和比较性分析。资源利用通过住院时间、器官支持和占用床日数来衡量。
712名患者符合纳入标准,其中172名(24%)接受了择期手术。其中,136名(19%)直接入住ICU,36名(5.1%)从病房非计划入院。择期手术患者占用了ICU患者总床日数的15.8%,其中44.3%是在非计划入院之后。与直接从手术室入院的患者相比,从病房非计划入院的择期手术患者疾病严重程度更高(急性生理与慢性健康状况评分系统II 17分对13分,p<0.01),需要呼吸或血管活性药物支持(75%对44%,p<0.01)以及医院死亡率更高(16.7%对2.2%,p<0.01)。
接受择期手术患者的ICU资源利用情况相当可观。那些直接从手术室入院的患者结局良好且资源利用低。从病房非计划入院的患者虽然数量较少,但病情更重,资源消耗更大,结局明显更差。