Department of Neurology, Xinqiao Hospital and The Second Affiliated Hospital, Army Medical University (Third Military Medical University), Chongqing, China.
Department of Neurology, Weifang Medical University, Weifang, China.
JAMA Netw Open. 2024 May 1;7(5):e249298. doi: 10.1001/jamanetworkopen.2024.9298.
The association of endovascular therapy (EVT) with outcomes is unclear for patients with very low Alberta Stroke Program Early Computed Tomography Score (ASPECTS) within 24 hours of stroke onset.
To explore the association of EVT with functional and safety outcomes among patients with ASPECTS of 0 to 2 scored with noncontrast computed tomography.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study used data from an ongoing, prospective, observational, nationwide registry including all patients treated at 38 stroke centers in China with an occlusion in the internal carotid artery or M1 or M2 segment of the middle cerebral artery within 24 hours of witnessed symptom onset. Patients with ASPECTS of 0 to 2 between November 1, 2021, and February 8, 2023, were included in analysis. Data were analyzed October to November 2023.
EVT vs standard medical treatment (SMT).
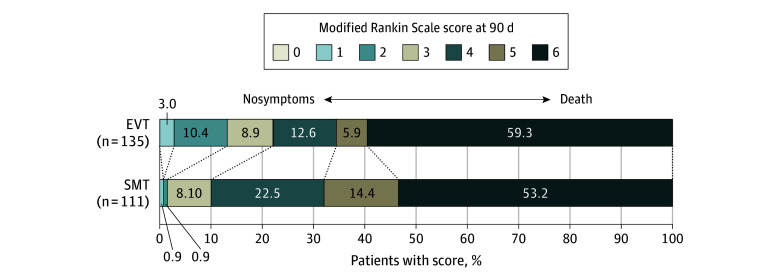
The primary outcome was favorable functional outcome, defined as modified Rankin Scale score (mRS) of 0 to 3, at 90 days. Safety outcomes included symptomatic intracerebral hemorrhage (sICH) within 48 hours and mortality at 90 days.
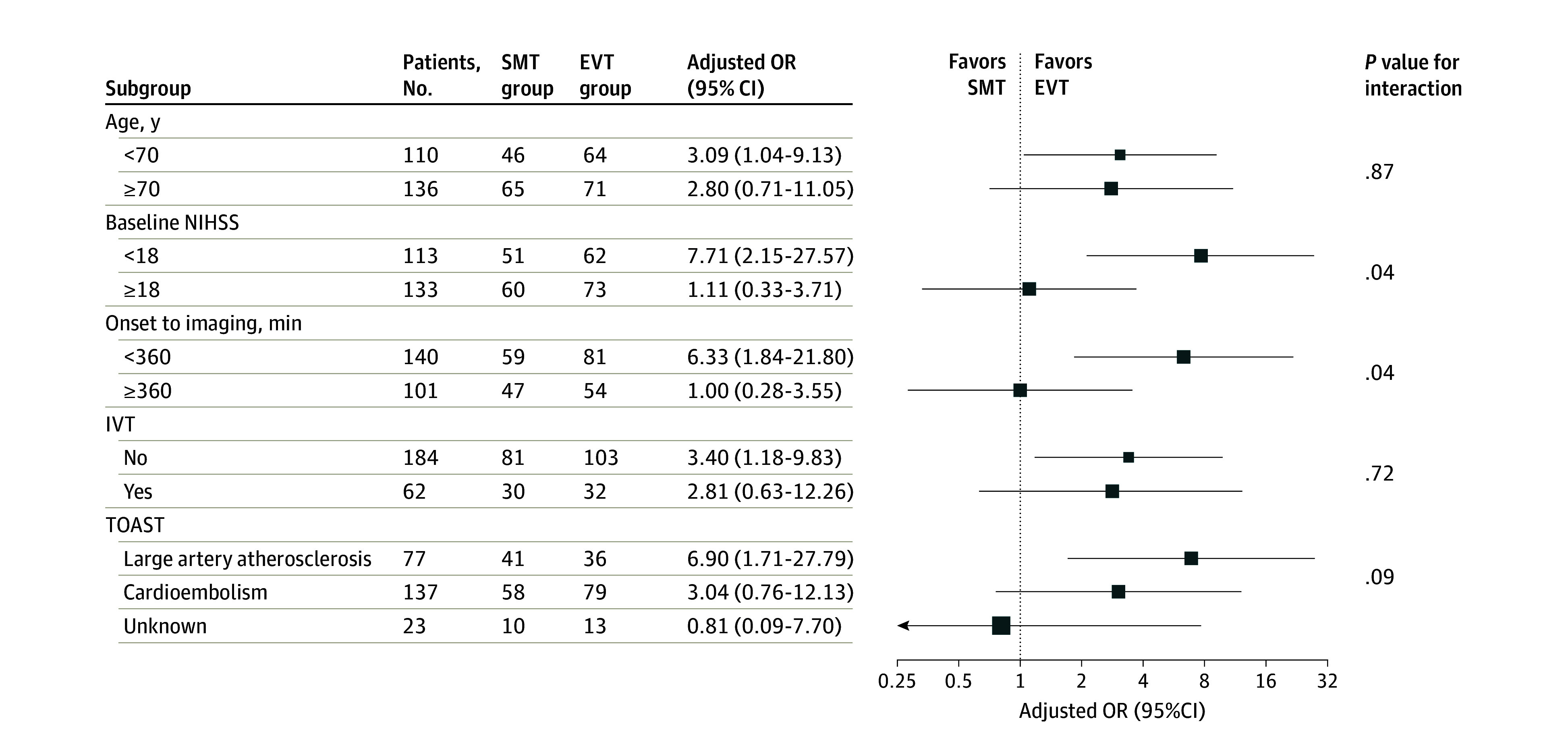
A total of 245 patients (median [IQR] age, 71 [63-78] years; 118 [48%] women) with ASPECTS of 0 to 2 were included, of whom 111 patients (45.1%) received SMT and 135 patients (54.9%) received EVT. The EVT group had significantly greater odds of favorable functional outcome at 90 days than the SMT group (30 patients [22.2%] vs 11 patients [9.9%]; P = .01; adjusted odds ratio [aOR], 3.07 [95% CI, 1.29-7.31]; P = .01). Patients in the EVT group, compared with the SMT group, had significantly greater odds of any ICH (56 patients [41.5%] vs 16 patients [11.4%]; P < .001; aOR, 4.27 [95% CI, 2.19-8.35]; P < .001) and sICH (24 patients [17.8%] vs 1 patient [0.9%]; P < .001; aOR, 23.07 [95% CI, 2.99-177.79]; P = .003) within 48 hours. There were no differences between groups for 90-day mortality (80 patients [59.3%] vs 59 patients [53.2%]; P = .34; aOR, 1.38 [95% CI, 0.77-2.47]; P = .28). The results remained robust in the propensity score-matched analysis.
In this cohort study of patients with very low ASPECTS based on NCCT within 24 hours of stroke onset, those treated with EVT had higher odds of a favorable functional outcome compared with those who received SMT. Randomized clinical trials are needed to assess these findings.
对于在卒中发病后 24 小时内 ASPECTS 评分 0 至 2 的患者,血管内治疗(EVT)与结局的关联尚不清楚。
探讨在接受非对比 CT 评分 ASPECTS 为 0 至 2 的患者中,EVT 与功能和安全性结局的关联。
设计、地点和参与者:这项队列研究使用了一项正在进行的、前瞻性、观察性的全国性注册研究的数据,该研究纳入了在中国 38 家卒中中心接受治疗的患者,这些患者在症状发作后 24 小时内有颈内动脉或大脑中动脉 M1 或 M2 段闭塞。2021 年 11 月 1 日至 2023 年 2 月 8 日之间 ASPECTS 评分为 0 至 2 的患者纳入分析。数据于 2023 年 10 月至 11 月进行分析。
EVT 与标准药物治疗(SMT)。
主要结局是 90 天时改良 Rankin 量表评分(mRS)为 0 至 3 的良好功能结局。安全性结局包括 48 小时内症状性颅内出血(sICH)和 90 天时的死亡率。
共纳入 245 例 ASPECTS 评分为 0 至 2 的患者(中位数[IQR]年龄 71[63-78]岁;118[48%]为女性),其中 111 例(45.1%)接受 SMT,135 例(54.9%)接受 EVT。与 SMT 组相比,EVT 组 90 天时功能结局良好的可能性显著更高(30 例[22.2%] vs 11 例[9.9%];P=0.01;调整后的优势比[aOR],3.07[95%CI,1.29-7.31];P=0.01)。与 SMT 组相比,EVT 组患者任何 ICH(56 例[41.5%] vs 16 例[11.4%];P<0.001;aOR,4.27[95%CI,2.19-8.35];P<0.001)和 sICH(24 例[17.8%] vs 1 例[0.9%];P<0.001;aOR,23.07[95%CI,2.99-177.79];P=0.003)的可能性显著更高。两组在 90 天死亡率方面没有差异(80 例[59.3%] vs 59 例[53.2%];P=0.34;aOR,1.38[95%CI,0.77-2.47];P=0.28)。在倾向评分匹配分析中,结果仍然稳健。
在这项基于卒中发病后 24 小时内 NCCT 的 ASPECTS 评分非常低的患者队列研究中,与接受 SMT 的患者相比,接受 EVT 的患者功能结局良好的可能性更高。需要进行随机临床试验来评估这些发现。