Department of Neurosurgery, West China Hospital, Sichuan University, Chengdu, Sichuan, China.
Department of Pharmacy, Institute of Metabolic Diseases and Pharmacotherapy, West China Hospital, Sichuan University, Chengdu, Sichuan, China.
Eur J Neurol. 2024 Aug;31(8):e16326. doi: 10.1111/ene.16326. Epub 2024 May 6.
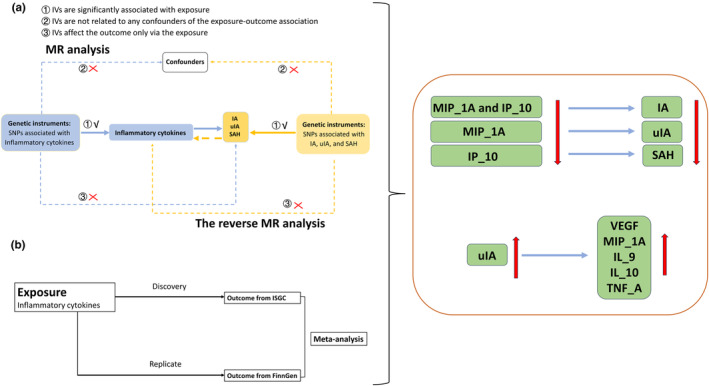
The causal association between inflammatory cytokines and the development of intracranial aneurysm (IA), unruptured IA (uIA) and subarachnoid hemorrhage (SAH) lacks clarity.
The summary-level datasets for inflammatory cytokines were extracted from a genome-wide association study of the Finnish Cardiovascular Risk in Young Adults Study and the FINRISK survey. The summary statistics datasets related to IA, uIA and SAH were obtained from the genome-wide association study meta-analysis of the International Stroke Genetics Consortium and FinnGen Consortium. The primary method employed for analysis was inverse variance weighting (false discovery rate), supplemented by sensitivity analyses to address pleiotropy and enhance robustness.
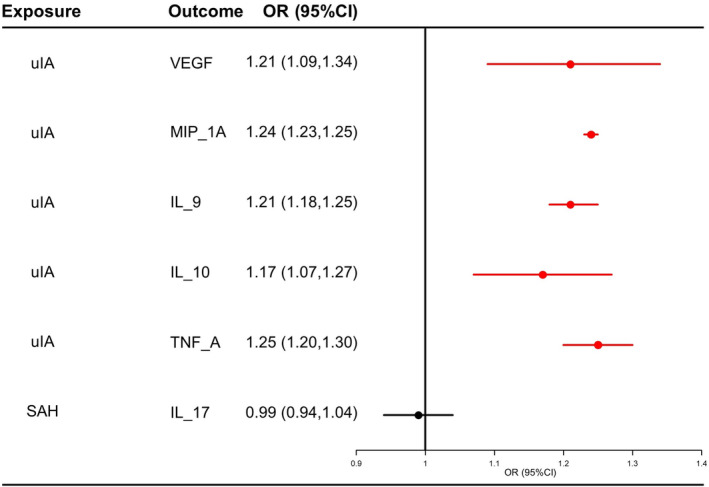
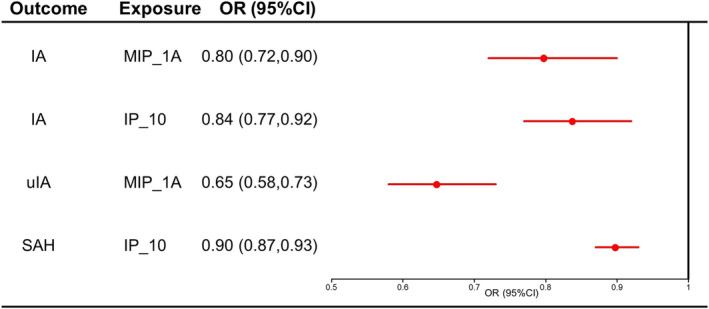
In the International Stroke Genetics Consortium, 10, six and eight inflammatory cytokines exhibited a causal association with IA, uIA and SAH, respectively (false discovery rate, p < 0.05). In FinnGen datasets, macrophage Inflammatory Protein-1 Alpha (MIP_1A), MIP_1A and interferon γ-induced protein 10 (IP_10) were verified for IA, uIA and SAH, respectively. In the reverse Mendelian randomization analysis, the common cytokines altered by uIA and SAH were vascular endothelial growth factor (VEGF), MIP_1A, IL_9, IL_10 and IL_17, respectively. The meta-analysis results show that MIP_1A and IP_10 could be associated with the decreased risk of IA, and MIP_1A and IP_10 were associated with the decreased risk of uIA and SAH, respectively. Notably, the levels of VEGF, MIP_1A, IL_9, IL_10 and TNF_A were increased with uIA. Comprehensive heterogeneity and pleiotropy analyses confirmed the robustness of these results.
Our study unveils a bidirectional association between inflammatory cytokines and IA, uIA and SAH. Further investigations are essential to validate their relationship and elucidate the underlying mechanisms.
炎症细胞因子与颅内动脉瘤(IA)、未破裂颅内动脉瘤(uIA)和蛛网膜下腔出血(SAH)的发展之间的因果关系尚不清楚。
从芬兰心血管风险在年轻人研究和芬兰风险调查的全基因组关联研究中提取炎症细胞因子的汇总数据集。与 IA、uIA 和 SAH 相关的汇总统计数据集来自国际中风遗传学联盟和芬兰基因联盟的全基因组关联研究荟萃分析。主要分析方法是逆方差加权(错误发现率),并辅以敏感性分析以解决多效性并增强稳健性。
在国际中风遗传学联盟中,有 10、6 和 8 种炎症细胞因子分别与 IA、uIA 和 SAH 存在因果关系(错误发现率,p < 0.05)。在芬兰基因数据集,巨噬细胞炎症蛋白-1α(MIP_1A)、MIP_1A 和干扰素γ诱导蛋白 10(IP_10)分别与 IA、uIA 和 SAH 相关。在反向孟德尔随机化分析中,uIA 和 SAH 改变的常见细胞因子分别为血管内皮生长因子(VEGF)、MIP_1A、IL_9、IL_10 和 IL_17。荟萃分析结果表明,MIP_1A 和 IP_10 可能与 IA 风险降低相关,MIP_1A 和 IP_10 分别与 uIA 和 SAH 风险降低相关。值得注意的是,VEGF、MIP_1A、IL_9、IL_10 和 TNF_A 的水平随着 uIA 的增加而升高。综合异质性和多效性分析证实了这些结果的稳健性。
本研究揭示了炎症细胞因子与 IA、uIA 和 SAH 之间的双向关联。需要进一步的研究来验证它们之间的关系并阐明潜在的机制。