Curtin School of Population Health, Curtin University, Kent Street, GPO Box U1987, Perth 6845, WA, Australia; Curtin Health Innovation Research Institute, Curtin University, Kent Street, GPO Box U1987, Perth 6845, Australia; School of Medical and Health Sciences, Edith Cowan University, 270 Joondalup Drive, Joondalup WA 6027, Australia.
School of Health Sciences, College of Health, Medicine and Wellbeing, University of Newcastle, Newcastle, Australia; Food and Nutrition Research Program, Hunter Medical Research Institute, New Lambton Heights, Newcastle, Australia.
Am J Clin Nutr. 2024 Jul;120(1):196-210. doi: 10.1016/j.ajcnut.2024.04.030. Epub 2024 May 6.
Technology-assisted 24-h dietary recalls (24HRs) have been widely adopted in population nutrition surveillance. Evaluations of 24HRs inform improvements, but direct comparisons of 24HR methods for accuracy in reference to a measure of true intake are rarely undertaken in a single study population.
To compare the accuracy of energy and nutrient intake estimation of 4 technology-assisted dietary assessment methods relative to true intake across breakfast, lunch, and dinner.
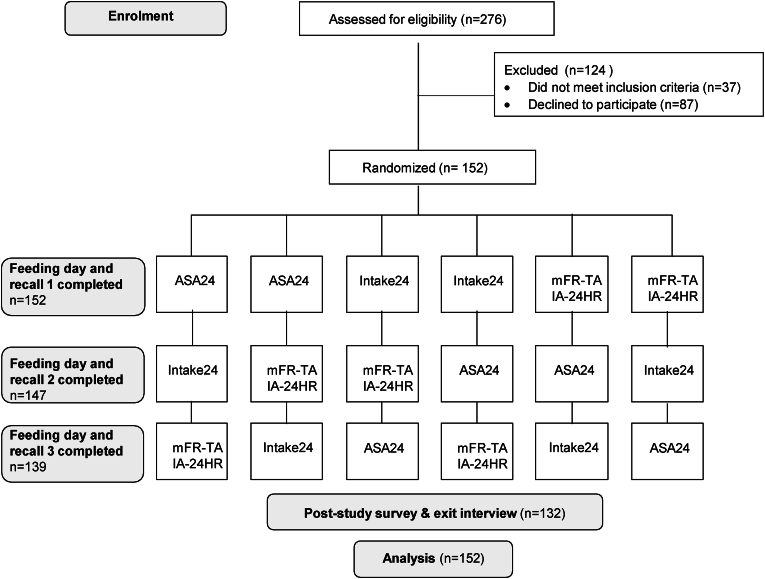
In a controlled feeding study with a crossover design, 152 participants [55% women; mean age 32 y, standard deviation (SD) 11; mean body mass index 26 kg/m, SD 5] were randomized to 1 of 3 separate feeding days to consume breakfast, lunch, and dinner, with unobtrusive weighing of foods and beverages consumed. Participants undertook a 24HR the following day [Automated Self-Administered Dietary Assessment Tool-Australia (ASA24); Intake24-Australia; mobile Food Record-Trained Analyst (mFR-TA); or Image-Assisted Interviewer-Administered 24-hour recall (IA-24HR)]. When assigned to IA-24HR, participants referred to images captured of their meals using the mobile Food Record (mFR) app. True and estimated energy and nutrient intakes were compared, and differences among methods were assessed using linear mixed models.
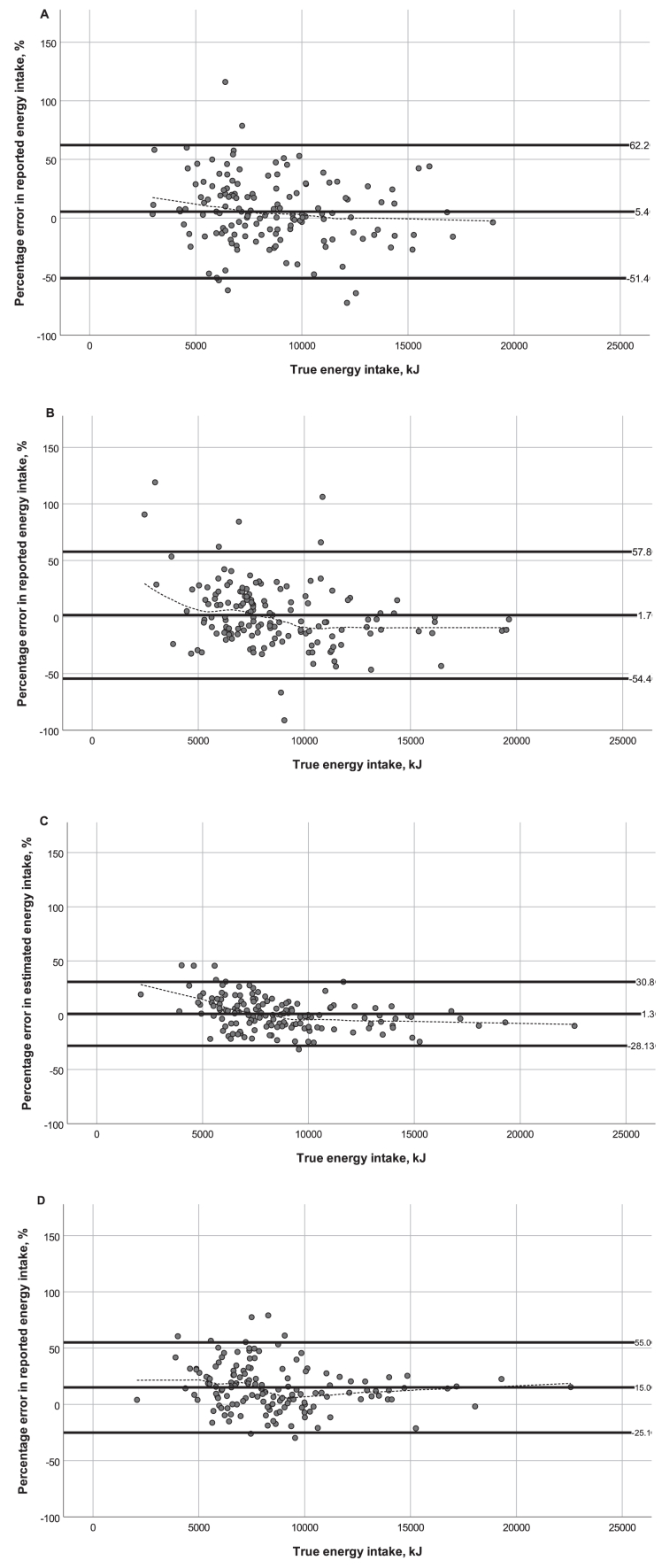
The mean difference between true and estimated energy intake as a percentage of true intake was 5.4% (95% CI: 0.6, 10.2%) using ASA24, 1.7% (95% CI: -2.9, 6.3%) using Intake24, 1.3% (95% CI: -1.1, 3.8%) using mFR-TA, and 15.0% (95% CI: 11.6, 18.3%) using IA-24HR. The variances of estimated and true energy intakes were statistically significantly different for all methods (P < 0.01) except Intake24 (P = 0.1). Differential accuracy in nutrient estimation was present among the methods.
Under controlled conditions, Intake24, ASA24, and mFR-TA estimated average energy and nutrient intakes with reasonable validity, but intake distributions were estimated accurately by Intake24 only (energy and protein). This study may inform considerations regarding instruments of choice in future population surveillance. This trial was registered at Australian New Zealand Clinical Trials Registry as ACTRN12621000209897.
技术辅助的 24 小时膳食回顾(24HR)已广泛应用于人群营养监测。对 24HR 的评估可以为改进提供信息,但很少在单个研究人群中进行针对真实摄入量的准确性的直接比较。
比较 4 种技术辅助膳食评估方法在早餐、午餐和晚餐时对能量和营养素摄入估计的准确性,以参考真实摄入量。
在一项具有交叉设计的对照喂养研究中,将 152 名参与者(55%为女性;平均年龄 32 岁,标准差 11;平均 BMI 为 26kg/m,标准差 5)随机分配到 3 个单独的喂养日中的 1 天,以食用早餐、午餐和晚餐,并对所食用的食物和饮料进行不显眼的称重。参与者在第二天进行 24HR(自动自我管理膳食评估工具-澳大利亚(ASA24);Intake24-澳大利亚;移动食物记录-培训分析师(mFR-TA);或图像辅助访谈者管理的 24 小时回忆(IA-24HR))。当被分配到 IA-24HR 时,参与者参考使用移动食物记录(mFR)应用程序拍摄的他们的膳食图像。比较真实和估计的能量和营养素摄入量,并使用线性混合模型评估方法之间的差异。
使用 ASA24 时,真实和估计能量摄入量的差异百分比为 5.4%(95%CI:0.6,10.2%),使用 Intake24 时为 1.7%(95%CI:-2.9,6.3%),使用 mFR-TA 时为 1.3%(95%CI:-1.1,3.8%),使用 IA-24HR 时为 15.0%(95%CI:11.6,18.3%)。除了 Intake24(P = 0.1)外,所有方法的估计和真实能量摄入量的方差均存在统计学显著差异(P < 0.01)。
在控制条件下,Intake24、ASA24 和 mFR-TA 可以合理地估计平均能量和营养素摄入量,但只有 Intake24(能量和蛋白质)才能准确估计摄入量分布。本研究可能为未来的人群监测提供有关工具选择的考虑。本试验在澳大利亚新西兰临床试验注册处注册,注册号为 ACTRN12621000209897。