Shoklo Malaria Research Unit (SMRU), Faculty of Tropical Medicine, Mahidol-Oxford Tropical Medicine Research Unit, Mahidol University Mae Sot, Bangkok, Thailand.
Centre for Tropical Medicine and Global Health, Nuffield Department of Medicine, University of Oxford, Oxford, OX3 7BN, UK.
Malar J. 2024 May 8;23(1):138. doi: 10.1186/s12936-024-04955-6.
Artemisinin resistance in Plasmodium falciparum threatens global malaria elimination efforts. To contain and then eliminate artemisinin resistance in Eastern Myanmar a network of community-based malaria posts was instituted and targeted mass drug administration (MDA) with dihydroartemisinin-piperaquine (three rounds at monthly intervals) was conducted. The prevalence of artemisinin resistance during the elimination campaign (2013-2019) was characterized.
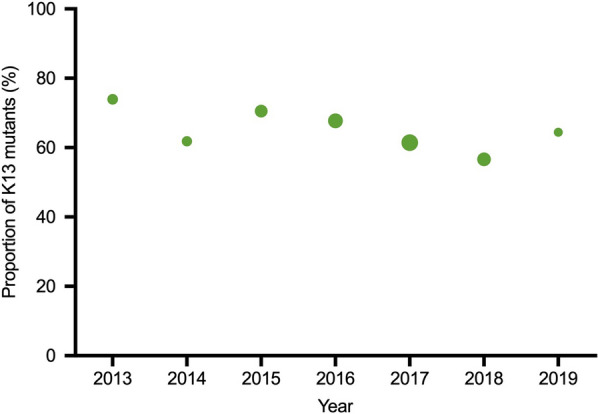
Throughout the six-year campaign Plasmodium falciparum positive blood samples from symptomatic patients and from cross-sectional surveys were genotyped for mutations in kelch-13-a molecular marker of artemisinin resistance.
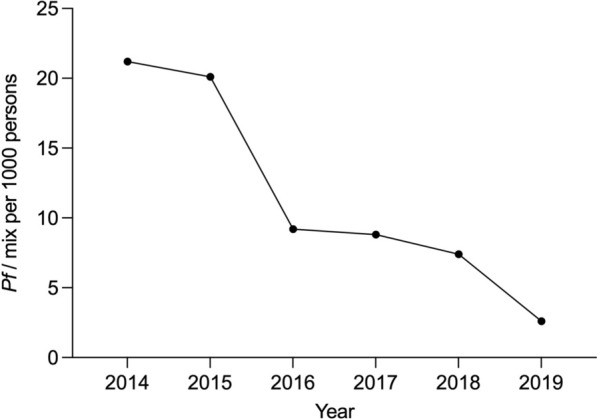
The program resulted in near elimination of falciparum malaria. Of 5162 P. falciparum positive blood samples genotyped, 3281 (63.6%) had K13 mutations. The prevalence of K13 mutations was 73.9% in 2013 and 64.4% in 2019. Overall, there was a small but significant decline in the proportion of K13 mutants (p < 0.001). In the MDA villages there was no significant change in the K13 proportions before and after MDA. The distribution of different K13 mutations changed substantially; F446I and P441L mutations increased in both MDA and non-MDA villages, while most other K13 mutations decreased. The proportion of C580Y mutations fell from 9.2% (43/467) before MDA to 2.3% (19/813) after MDA (p < 0.001). Similar changes occurred in the 487 villages where MDA was not conducted.
The malaria elimination program in Kayin state, eastern Myanmar, led to a substantial reduction in falciparum malaria. Despite the intense use of artemisinin-based combination therapies, both in treatment and MDA, this did not select for artemisinin resistance.
恶性疟原虫对青蒿素的抗药性对全球疟疾消除工作构成威胁。为了遏制并最终消除缅甸东部的青蒿素抗药性,建立了一个以社区为基础的疟疾监测点网络,并进行了以双氢青蒿素-哌喹(每月间隔三轮)为基础的靶向大规模药物治疗(MDA)。本研究描述了在消除运动期间(2013-2019 年)青蒿素耐药性的流行情况。
在六年的运动期间,对来自症状性患者和横断面调查的疟原虫阳性血样进行kelch-13a 基因突变的基因分型,kelch-13a 是青蒿素耐药性的分子标志物。
该方案导致恶性疟原虫的几乎消除。在 5162 份疟原虫阳性血样中,3281 份(63.6%)存在 kelch-13 基因突变。2013 年 K13 突变的流行率为 73.9%,2019 年为 64.4%。总体而言,K13 突变体的比例略有下降,但具有统计学意义(p<0.001)。在 MDA 村,MDA 前后 K13 比例没有显著变化。不同 K13 突变的分布发生了很大变化;F446I 和 P441L 突变在 MDA 和非 MDA 村都有所增加,而大多数其他 K13 突变则减少。C580Y 突变的比例从 MDA 前的 9.2%(43/467)降至 MDA 后的 2.3%(19/813)(p<0.001)。在没有进行 MDA 的 487 个村庄中也发生了类似的变化。
缅甸克钦邦的疟疾消除计划导致恶性疟的大幅减少。尽管在治疗和 MDA 中大量使用了青蒿素为基础的联合疗法,但并没有选择出青蒿素耐药性。