Li Bing, Chen Yu, Ma Rong
Department of Anesthesiology, Jiangsu Province Hospital and First Affiliated Hospital with Nanjing Medical University, Nanjing City, China.
Interdiscip Cardiovasc Thorac Surg. 2024 May 2;38(5). doi: 10.1093/icvts/ivae096.
The aim of this study was to evaluate the efficacy of a multimodal preemptive analgesia management approach, specifically incorporating ultrasound-guided thoracic paravertebral block (UG-TPVB) in conjunction with intravenous analgesia, after video-assisted thoracoscopic (VATS) lobectomy under the guidance of enhanced recovery after surgery.
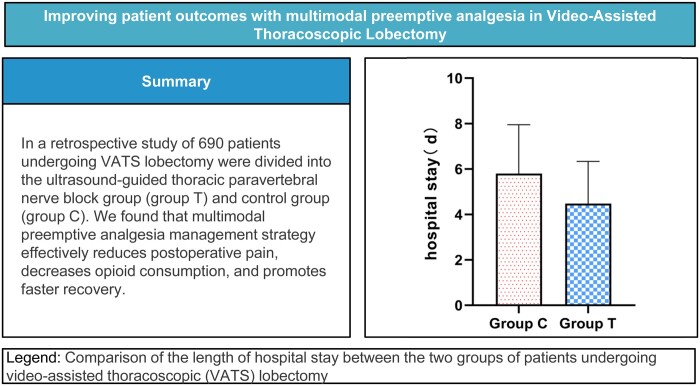
A total of 690 patients who underwent VATS lobectomy between October 2021 and March 2022 were divided into the UG-TPVB group (group T, n = 345) and the control group (group C, n = 345). Patients in group T received UG-TPVB prior to the induction of general anaesthesia, while group C did not undergo nerve block. A comparison was conducted between the 2 groups regarding various indicators, including postoperative sedation, static/dynamic numeric rating scale scores, intraoperative fentanyl consumption, duration of mechanical ventilation/anaesthesia recovery/hospitalization, postoperative complications and other relevant factors.
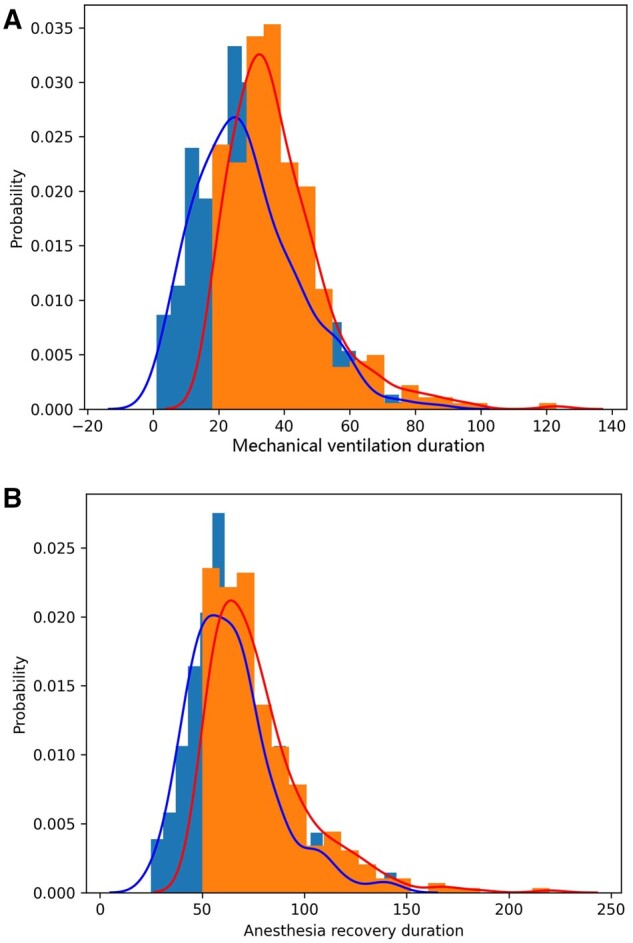
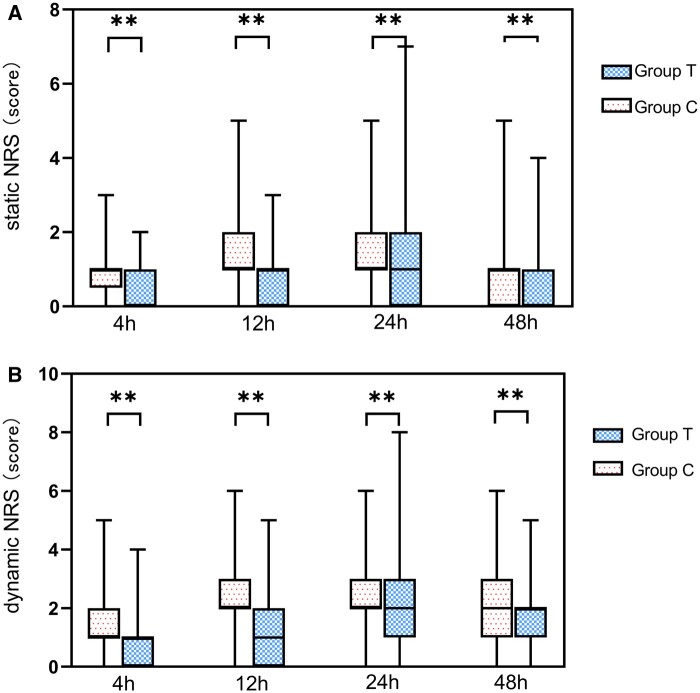
The static/dynamic numeric rating scale scores of group T were lower than those of group C after surgery. Intraoperative fentanyl consumption in group T (0.384 ± 0.095 mg) was lower than that in group C (0.465 ± 0.053 mg). The duration of mechanical ventilation, anaesthesia recovery and hospitalization were significantly shorter in group T compared to group C. Patient satisfaction rate in group T (70.1%) was higher than that in group C (53.6%). All differences were statistically significant (P < 0.05).
The multimodal preemptive analgesia management strategy effectively reduces postoperative pain, decreases opioid consumption and promotes faster recovery in patients undergoing VATS lobectomy.
本研究旨在评估一种多模式超前镇痛管理方法的疗效,特别是在术后加速康复指导下,将超声引导下胸椎旁神经阻滞(UG-TPVB)与静脉镇痛相结合,应用于电视辅助胸腔镜(VATS)肺叶切除术后。
将2021年10月至2022年3月期间接受VATS肺叶切除术的690例患者分为UG-TPVB组(T组,n = 345)和对照组(C组,n = 345)。T组患者在全身麻醉诱导前接受UG-TPVB,而C组未进行神经阻滞。比较两组在术后镇静、静态/动态数字评分量表得分、术中芬太尼用量、机械通气/麻醉恢复/住院时间、术后并发症及其他相关因素等各项指标。
术后T组的静态/动态数字评分量表得分低于C组。T组术中芬太尼用量(0.384±0.095mg)低于C组(0.465±0.053mg)。与C组相比,T组的机械通气、麻醉恢复和住院时间明显缩短。T组患者满意度(70.1%)高于C组(53.6%)。所有差异均有统计学意义(P < 0.05)。
多模式超前镇痛管理策略可有效减轻VATS肺叶切除术后患者的疼痛,减少阿片类药物用量,并促进患者更快康复。