Feng Man, Wang Lulu, Sun Jing, Chen Zheping, Fu Jia, Liu Dongyi, Zhang Rumeng, Li Youqin, Zhang Yan, Zhang He, Zhang Weiquan, Feng Chang
Department of Pathology, Affiliated Hospital of Shandong Academy of Medical Sciences, The third Affiliated Hospital of Shandong First Medical University, Jinan, 250000, People's Republic of China.
Cheeloo College of Medicine, Shandong University, Jinan, 250033, People's Republic of China.
Cancer Manag Res. 2022 Mar 3;14:953-965. doi: 10.2147/CMAR.S346285. eCollection 2022.
To investigate the effects of ultrasound-guided thoracic paravertebral block combined with general anaesthesia or general anaesthesia alone for thoracoscopic lung adenocarcinoma surgery, and to provide new thoughts for improving the clinical outcomes.
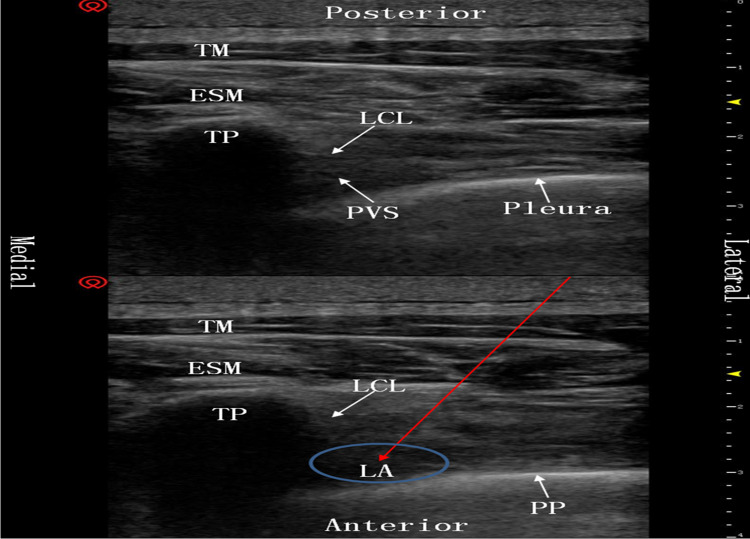
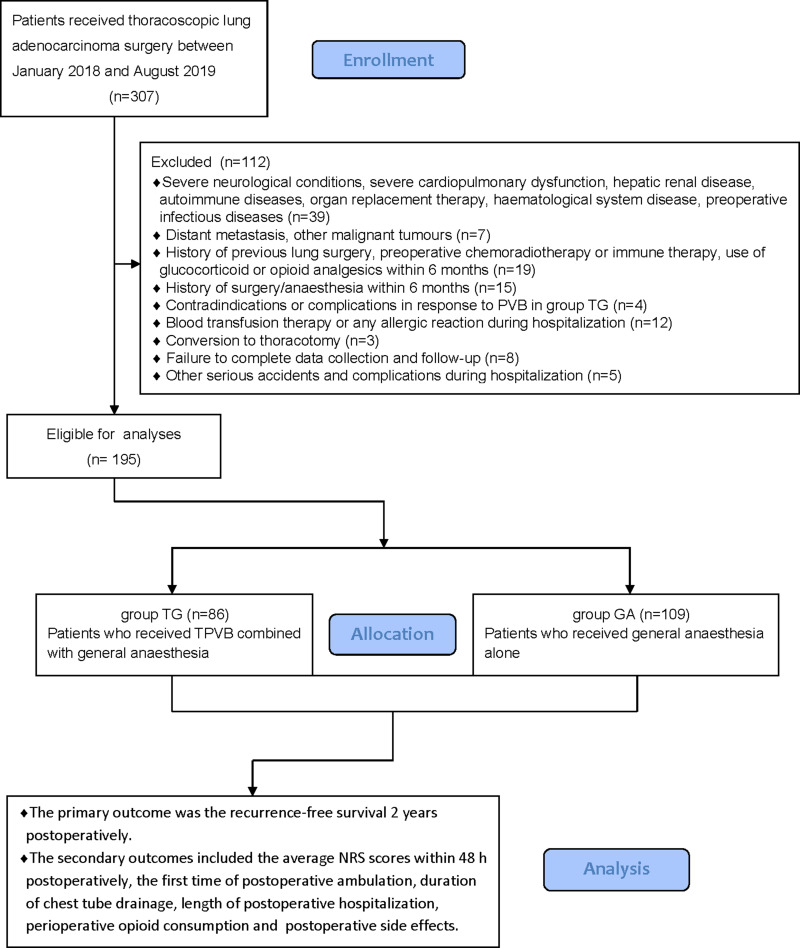
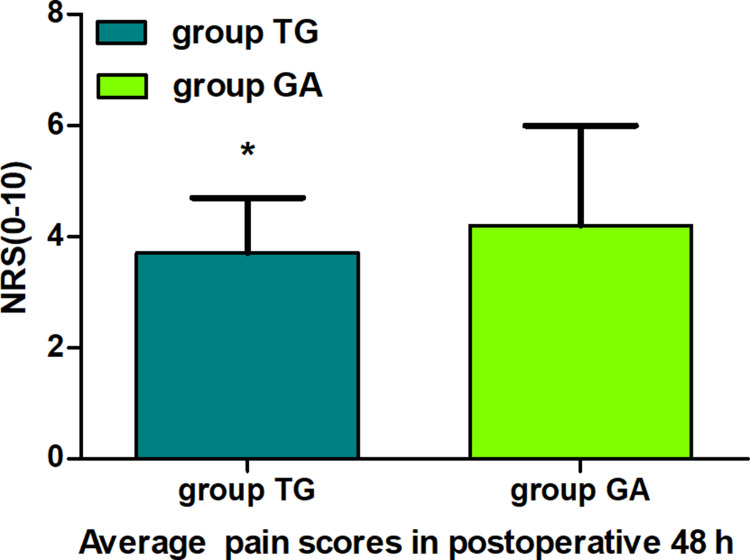
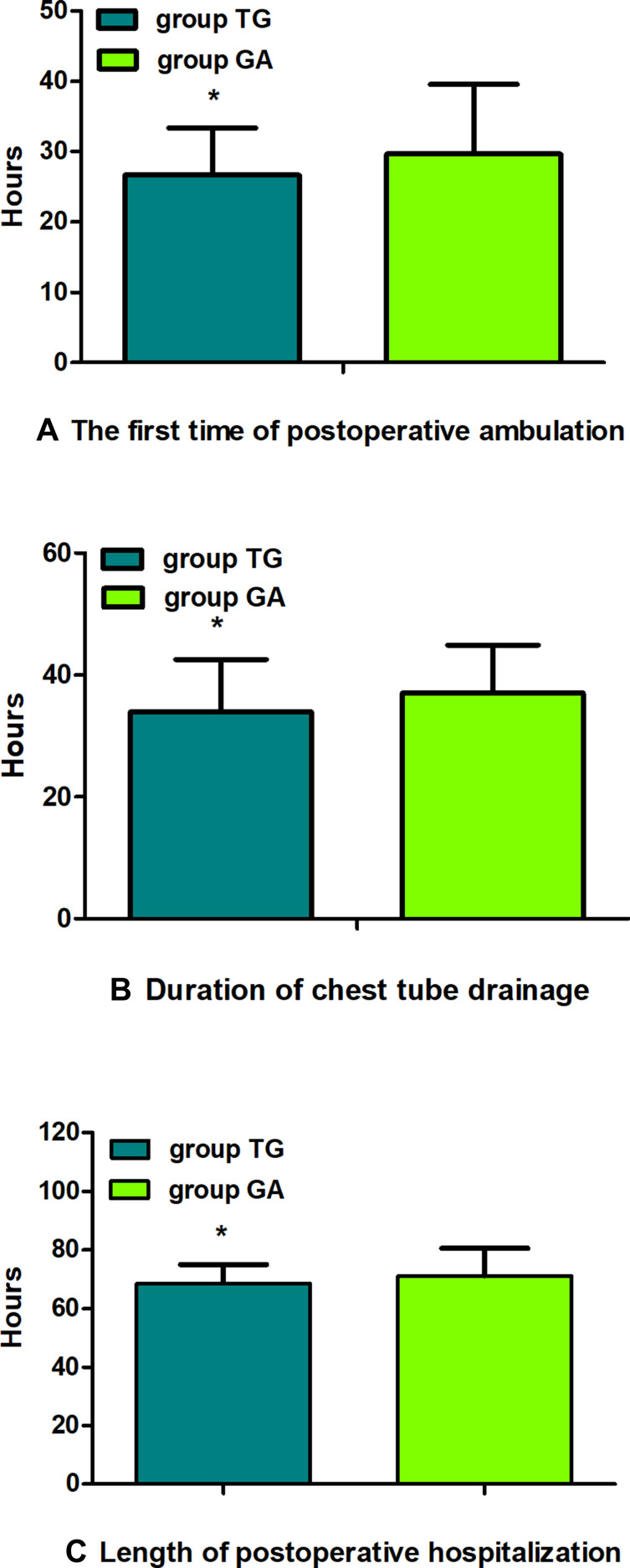
This was a retrospective study. Data were retrieved for 195 patients with lung adenocarcinoma undergoing elective radical lobectomy via video-assisted thoracoscopy between January 2018 and August 2019 in The Second Hospital of Shandong University, including 86 patients who received thoracic paravertebral block (TPVB) combined with general anaesthesia (group TG), and 109 patients who received general anaesthesia alone (group GA). All patients were given self-controlled intravenous analgesia pump for 48 h after surgery. The primary outcome was the recurrence-free survival 2 years postoperatively (the time between surgery and the earliest date of recurrence, metastasis or lung cancer-cause death). The secondary outcomes included the average numeric rating scale (NRS) scores within 48 h postoperatively, the first time of postoperative ambulation, duration of chest tube drainage, length of postoperative hospitalization, perioperative opioid consumption and the postoperative side effects.
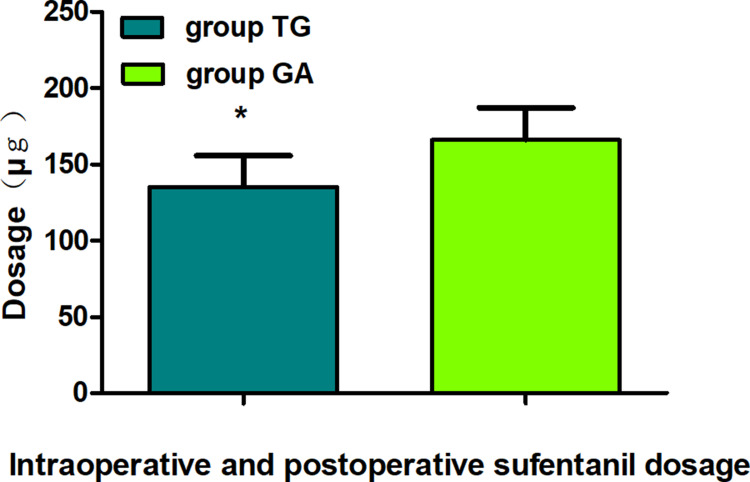
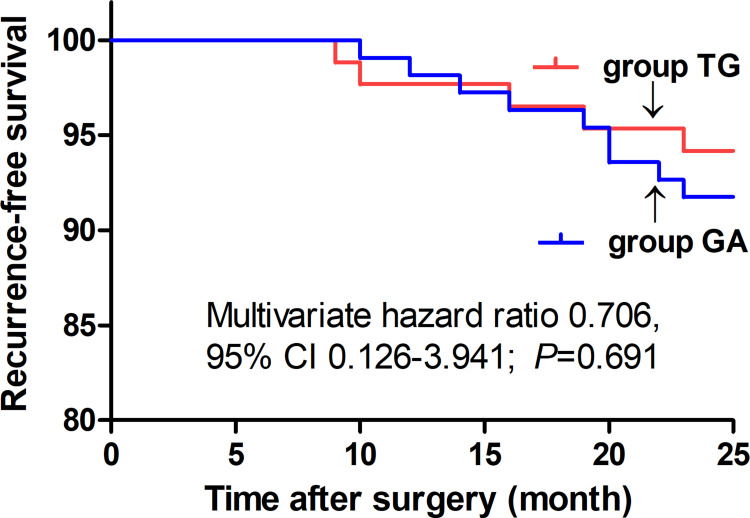
There were no statistical differences in the recurrence-free survival 2 years postoperatively between groups (Multivariate hazard ratio 0.706, 95% CI 0.126-3.941, =0.691). The average NRS scores within 48 h postoperatively were significantly lower in group TG (<0.05). The first time of postoperative ambulation, duration of chest tube drainage, and length of postoperative hospitalization in group TG were significantly reduced (<0.05). Opioid consumption was significantly decreased in group TG (<0.01). Finally, the incidence of postoperative nausea and vomiting (PONV) was significantly lower in group TG (<0.05).
TPVB for thoracoscopic lung adenocarcinoma surgery did not improve the recurrence-free survival 2 years postoperatively compared with general anaesthesia alone, but it significantly enhanced the postoperative analgesia effect, reduced opioid consumption as well as side effects, and accelerated postoperative early recovery.
The Chinese Clinical Trial Registry (ChiCTR-2100050454).
探讨超声引导下胸椎旁神经阻滞联合全身麻醉与单纯全身麻醉用于胸腔镜肺腺癌手术的效果,为改善临床结局提供新思路。
本研究为回顾性研究。收集2018年1月至2019年8月在山东大学第二医院行择期电视辅助胸腔镜根治性肺叶切除术的195例肺腺癌患者的数据,其中86例接受胸椎旁神经阻滞(TPVB)联合全身麻醉(TG组),109例接受单纯全身麻醉(GA组)。所有患者术后均给予自控静脉镇痛泵48小时。主要结局为术后2年无复发生存期(手术至复发、转移或肺癌相关死亡的最早日期之间的时间)。次要结局包括术后48小时内的平均数字评定量表(NRS)评分、术后首次下床活动时间、胸腔闭式引流时间、术后住院时间、围手术期阿片类药物消耗量及术后副作用。
两组术后2年无复发生存期无统计学差异(多因素风险比0.706,95%可信区间0.126 - 3.941,P = 0.691)。TG组术后48小时内的平均NRS评分显著更低(P<0.05)。TG组术后首次下床活动时间、胸腔闭式引流时间及术后住院时间显著缩短(P<0.05)。TG组阿片类药物消耗量显著减少(P<0.01)。最后,TG组术后恶心呕吐(PONV)发生率显著更低(P<0.05)。
与单纯全身麻醉相比,TPVB用于胸腔镜肺腺癌手术并未改善术后2年无复发生存期,但显著增强了术后镇痛效果,减少了阿片类药物消耗量及副作用,并加速了术后早期恢复。
中国临床试验注册中心(ChiCTR-2100050454)