Sarad Nakia, Basilious Mark, Nag Uttara, Jethmalani Nitin, Agrusa Christopher, Ellozy Sharif, DeRubertis Brian, Connolly Peter
Division of Vascular and Endovascular Surgery, Weill Cornell Medical College, NewYork-Presbyterian Hospital, New York, NY.
J Vasc Surg Cases Innov Tech. 2024 Apr 3;10(4):101499. doi: 10.1016/j.jvscit.2024.101499. eCollection 2024 Aug.
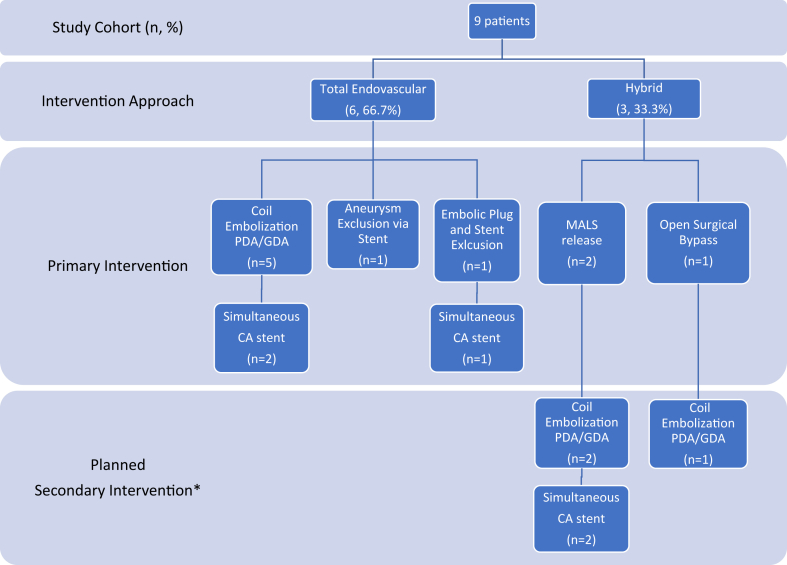
True aneurysms of the pancreaticoduodenal artery (PDA) arcade are rare but require intervention due to the high risk of rupture. Historically, these aneurysms have been managed with open surgical methods. In this study, we describe a contemporary series of aneurysms treated using a modern approach that includes endovascular and hybrid techniques. All the patients with aneurysms of the PDA arcade in an institutional database were identified between 2008 and 2022. Patients with history of pancreatic resection were excluded. Data on demographics, presenting symptoms, imaging findings, operative approach, and outcomes were collected and reviewed. There were nine patients diagnosed with a PDA aneurysm, and all nine underwent endovascular intervention. Most were men (n = 5; 55.6%) and White (n = 7; 77.8%) and had American Society of Anesthesiologists class II or III. The median aneurysm size was 21 mm (range, 6-42 mm), and five (55.5%) were symptomatic. Of the five symptomatic cases, two presented with rupture and were treated urgently. The median time to intervention for the nonurgent cases was 30 days. All but one patient had concomitant celiac artery stenosis and two of the eight cases (25%) were due to extrinsic compression from median arcuate ligament syndrome. Both patients underwent median arcuate ligament syndrome release before endovascular intervention. Another patient required open surgical bypass before endovascular repair from the supraceliac aorta to hepatic artery using a Dacron graft to maintain hepatic perfusion. Among the eight patients with celiac axis stenosis, five (62.5%) required celiac stent placement within the same operation. Coil embolization of the aneurysm was used for all except for two patients (n = 7 of 9; 77.8%), with one patient receiving embolic plugs and another receiving an 8 × 38-mm balloon-expandable covered stent for aneurysm exclusion. The median operating room time was 134 minutes. All repairs were technically successful without any intraoperative or postoperative complications. The mean follow-up was 30 months. There was no morbidity, mortality, or unplanned secondary reinterventions within 6 months after aneurysm repair. Stent patency and aneurysm size remained stable at 2 years of follow-up. True pancreaticoduodenal artery arcade aneurysms can be safely and effectively treated using endovascular and hybrid techniques. Because many of these aneurysms have concomitant celiac artery stenosis, the use of endovascular technology allows for simultaneous treatment of both the aneurysm and the stenosis with exceptional results.
胰十二指肠动脉弓真性动脉瘤罕见,但因破裂风险高而需要干预。历史上,这些动脉瘤一直采用开放手术方法治疗。在本研究中,我们描述了一系列采用现代方法治疗的动脉瘤,包括血管内和杂交技术。在一个机构数据库中识别出2008年至2022年间所有患有胰十二指肠动脉弓动脉瘤的患者。排除有胰腺切除术史的患者。收集并回顾了人口统计学、临床表现、影像学检查结果、手术方法及预后等数据。有9例患者被诊断为胰十二指肠动脉弓动脉瘤,均接受了血管内介入治疗。大多数为男性(n = 5;55.6%),白人(n = 7;77.8%),美国麻醉医师协会分级为II或III级。动脉瘤中位大小为21 mm(范围6 - 42 mm),5例(55.5%)有症状。在这5例有症状的病例中,2例出现破裂并接受了紧急治疗。非紧急病例的中位干预时间为30天。除1例患者外,所有患者均伴有腹腔干狭窄,8例中有2例(25%)是由于正中弓状韧带综合征的外在压迫所致。这2例患者在血管内介入治疗前均接受了正中弓状韧带松解术。另1例患者在血管内修复前需要行开放手术搭桥,即从腹腔干上方主动脉至肝动脉使用涤纶移植物以维持肝灌注。在8例有腹腔干狭窄的患者中,5例(62.5%)在同一手术中需要放置腹腔干支架。除2例患者外,所有患者均采用动脉瘤弹簧圈栓塞治疗(9例中的7例,77.8%),1例患者接受栓塞栓子治疗,另1例患者接受8×38 mm球囊扩张式覆膜支架以排除动脉瘤。中位手术时间为134分钟。所有修复技术均成功,无任何术中或术后并发症。平均随访30个月。动脉瘤修复后6个月内无发病率、死亡率或计划外二次干预情况。随访2年时,支架通畅情况及动脉瘤大小保持稳定。采用血管内和杂交技术可安全有效地治疗真性胰十二指肠动脉弓动脉瘤。由于这些动脉瘤中有许多伴有腹腔干狭窄,血管内技术的应用可同时治疗动脉瘤和狭窄,效果极佳。