Department of Cardiovascular Medicine, University of Tennessee Health Science Center College of Medicine-Chattanooga, Chattanooga, Tennessee, United States of America.
Department of Cardiovascular Medicine, Columbia University Medical Center, New York, NY, United States of America.
PLoS One. 2024 May 21;19(5):e0302378. doi: 10.1371/journal.pone.0302378. eCollection 2024.
Guidelines recommend shared decision making when choosing treatment for severe aortic stenosis but implementation has lagged. We assessed the feasibility and impact of a novel decision aid for severe aortic stenosis at point-of-care.
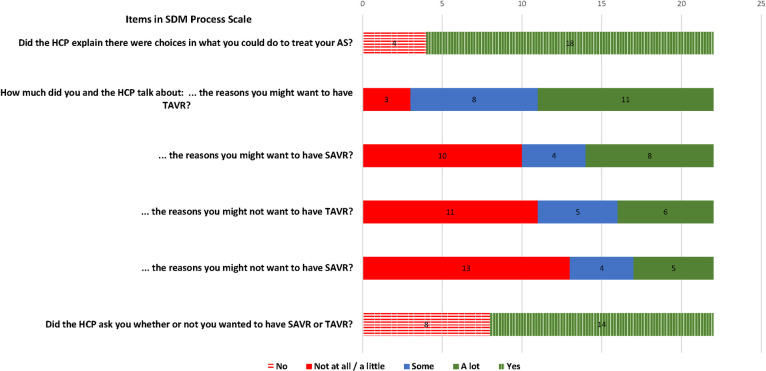
This prospective multi-site pilot cohort study included adults with severe aortic stenosis and their clinicians. Patients were referred by their heart team when scheduled to discuss treatment options. Outcomes included shared decision-making processes, communication quality, decision-making confidence, decisional conflict, knowledge, stage of decision making, decision quality, and perceptions of the tool. Patients were assessed at baseline (T0), after using the intervention (T1), and after the clinical encounter (T2); clinicians were assessed at T2. Before the encounter, patients reviewed the intervention, Aortic Valve Improved Treatment Approaches (AVITA), an interactive, online decision aid. AVITA presents options, frames decisions, clarifies patient goals and values, and generates a summary to use with clinicians during the encounter.
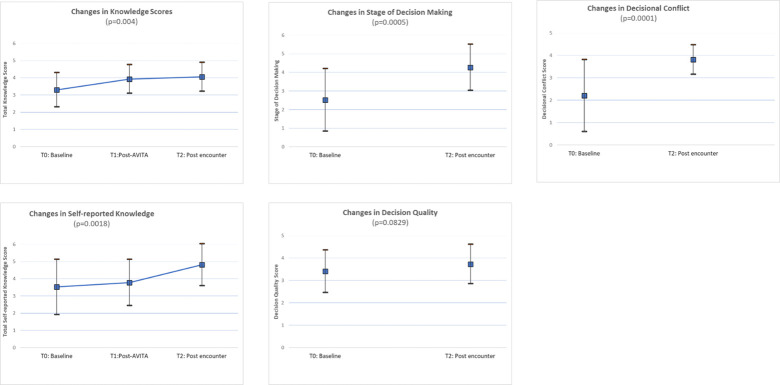
30 patients (9 women [30.0%]; mean [SD] age 70.4 years [11.0]) and 14 clinicians (4 women [28.6%], 7 cardiothoracic surgeons [50%]) comprised 28 clinical encounters Most patients [85.7%] and clinicians [84.6%] endorsed AVITA. Patients reported AVITA easy to use [89.3%] and helped them choose treatment [95.5%]. Clinicians reported the AVITA summary helped them understand their patients' values [80.8%] and make values-aligned recommendations [61.5%]. Patient knowledge significantly improved at T1 and T2 (p = 0.004). Decisional conflict, decision-making stage, and decision quality improved at T2 (p = 0.0001, 0.0005, and 0.083, respectively). Most patients [60%] changed treatment preference between T0 and T2. Initial treatment preferences were associated with low knowledge, high decisional conflict, and poor decision quality; final preferences were associated with high knowledge, low conflict, and high quality.
AVITA was endorsed by patients and clinicians, easy to use, improved shared decision-making quality and helped patients and clinicians arrive at a treatment that reflected patients' values.
Trial ID: NCT04755426, Clinicaltrials.gov/ct2/show/NCT04755426.
指南建议在选择严重主动脉瓣狭窄的治疗方法时采用共同决策,但实施情况滞后。我们评估了一种新型严重主动脉瓣狭窄即时决策辅助工具的可行性和影响。
这是一项前瞻性多地点试点队列研究,纳入了严重主动脉瓣狭窄患者及其临床医生。当心脏团队安排讨论治疗选择时,患者将由其转诊。研究结果包括共同决策过程、沟通质量、决策信心、决策冲突、知识、决策阶段、决策质量和对工具的看法。患者在基线(T0)、使用干预措施后(T1)和临床就诊后(T2)进行评估;临床医生在 T2 时进行评估。在就诊前,患者查看了干预措施,即主动脉瓣改善治疗方法(AVITA),这是一种交互式在线决策辅助工具。AVITA 提供了多种选择,对决策进行了阐述,明确了患者的目标和价值观,并生成了一份总结,以便在就诊时与临床医生一起使用。
共有 30 名患者(9 名女性[30.0%];平均[标准差]年龄 70.4 岁[11.0])和 14 名临床医生(4 名女性[28.6%],7 名心胸外科医生[50%])组成了 28 次临床就诊。大多数患者[85.7%]和临床医生[84.6%]对 AVITA 表示认可。患者报告说 AVITA 易于使用[89.3%],并帮助他们选择了治疗方法[95.5%]。临床医生报告说,AVITA 总结有助于他们了解患者的价值观[80.8%]并提出符合价值观的建议[61.5%]。患者的知识在 T1 和 T2 时显著提高(p = 0.004)。决策冲突、决策阶段和决策质量在 T2 时得到改善(p = 0.0001、0.0005 和 0.083)。大多数患者[60%]在 T0 和 T2 之间改变了治疗偏好。初始治疗偏好与低知识、高决策冲突和低决策质量相关;最终偏好与高知识、低冲突和高质量相关。
AVITA 得到了患者和临床医生的认可,易于使用,提高了共同决策的质量,并帮助患者和临床医生制定了反映患者价值观的治疗方案。
试验 ID:NCT04755426,Clinicaltrials.gov/ct2/show/NCT04755426。