Ushioda Ryohei, Hirofuji Aina, Yoongtong Dit, Sakboon Boonsap, Cheewinmethasiri Jaroen, Lokeskrawee Thanin, Patumanond Jayanton, Lawanaskol Suppachai, Kamiya Hiroyuki, Arayawudhikul Nuttapon
Cardiovascular and Thoracic Surgery Unit, Department of Surgery, Lampang Hospital, Lampang, Thailand.
Department of Cardiac Surgery, Asahikawa Medical University, Asahikawa, Japan.
Front Cardiovasc Med. 2024 May 7;11:1391881. doi: 10.3389/fcvm.2024.1391881. eCollection 2024.
At our institution, we perform off-pump coronary artery bypass (OPCAB) as a standard procedure. Moreover, patients with favorable coronary anatomy and condition are selected for minimally invasive cardiac surgery (MICS)-OPCAB. We retrospectively compared early outcomes, focusing on safety, between MICS-OPCAB and conventional off-pump techniques for multivessel coronary artery bypass grafting (CABG).
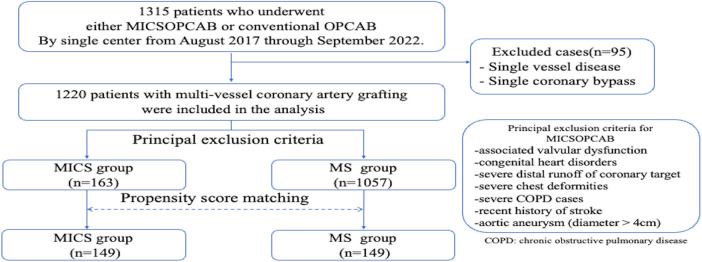
From August 2017 to September 2022, 1,220 patients underwent multivessel coronary artery grafting at our institution. They were divided into the MICS-OPCAB group (MICS group = 163 patients) and the conventional OPCAB group (MS group = 1057 patients). Propensity score matching (1 : 1 ratio) was applied to the MICS-OPCAB and MS groups (149 patients per group) based on 23 preoperative clinical characteristics.
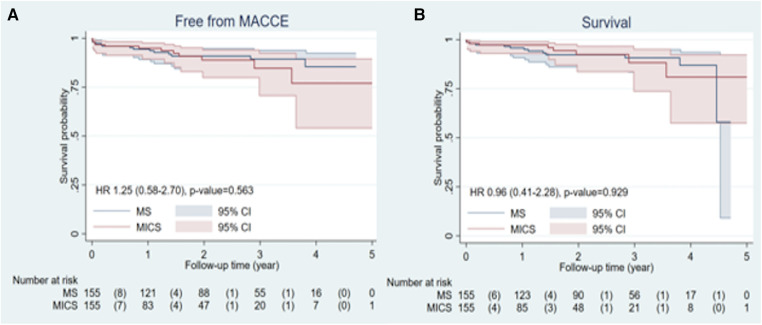
After matching, there were no significant differences in preoperative characteristics between the groups. The MICS group had a lower total graft number (2.3 ± 0.6 vs. 2.9 ± 0.8, < 0.001) and fewer distal anastomoses (2.7 ± 0.8 vs. 3.2 ± 0.9, < 0.001). There were no significant differences in hospital stay, intensive care unit stay, postoperative complications, and 30-day mortality. The MICS group had less drain output (MICS 350 ml [250-500], MS 450 ml [300-550]; = 0.013). Kaplan-Meier analysis revealed no significant differences in postoperative MACCE (major adverse cardiac or cerebrovascular events)-free and survival rates between the groups (MACCE-free rate = 0.945, survival rate = 0.374).
With proper patient selection, MICS-OPCAB can provide good short to mid-term results, similar to those of conventional OPCAB.
在我们机构,非体外循环冠状动脉搭桥术(OPCAB)是一项标准手术。此外,冠状动脉解剖结构和状况良好的患者被选用于微创心脏手术(MICS)-OPCAB。我们回顾性比较了MICS-OPCAB与多支冠状动脉搭桥术(CABG)的传统非体外循环技术在早期结果方面的差异,重点关注安全性。
2017年8月至2022年9月,1220例患者在我们机构接受了多支冠状动脉搭桥术。他们被分为MICS-OPCAB组(MICS组 = 163例患者)和传统OPCAB组(MS组 = 1057例患者)。基于23项术前临床特征,对MICS-OPCAB组和MS组(每组149例患者)进行倾向评分匹配(1:1比例)。
匹配后,两组术前特征无显著差异。MICS组的总移植血管数较少(2.3±0.6对2.9±0.8,<0.001),远端吻合口较少(2.7±0.8对3.2±0.9,<0.001)。住院时间、重症监护病房停留时间、术后并发症和30天死亡率无显著差异。MICS组的引流量较少(MICS 350 ml [250 - 500],MS 450 ml [300 - 550]; = 0.013)。Kaplan-Meier分析显示,两组术后无主要不良心脏或脑血管事件(MACCE)生存率和总生存率无显著差异(无MACCE生存率 = 0.945,生存率 = 0.374)。
通过适当的患者选择,MICS-OPCAB可以提供与传统OPCAB相似的良好短期至中期结果。