Department of Neurology, Xuanwu Hospital, Capital Medical University, No. 45 Changchun Street, Xicheng District, Beijing, 100053, China.
National Clinical Research Center for Geriatric Disorders, Beijing, China.
Sci Rep. 2024 May 23;14(1):11773. doi: 10.1038/s41598-024-62092-1.
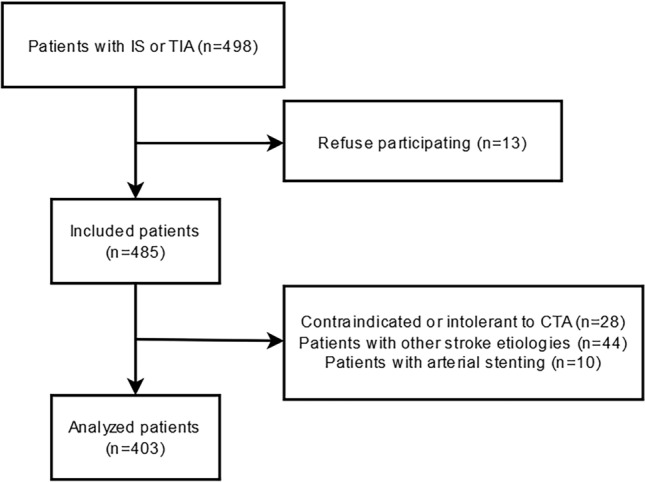
Patients with ischemic cerebrovascular disease (ICVD) frequently develop concomitant peripheral artery disease (PAD) or renal artery stenosis (RAS), and multiterritorial atherosclerotic patients usually have a worse prognosis. We aimed to evaluate the status of peripheral atherosclerosis (AS) and cervicocephalic AS (CAS) in ICVD patients with AS, their correlation, and related risk factors contributing to coexisting cervicocephalic-peripheral AS (CPAS). Based on the severity and extent of AS evaluated by computed tomography angiography and ultrasound, the degree of AS was triple categorized to assess the correlation between CAS and PAD/RAS. CAS and PAD/RAS were defined as the most severe stenosis being ≥ 50% luminal diameter in cervicocephalic or lower limb arteries, and a peak systolic velocity at the turbulent site being ≥ 180 cm/s in the renal artery. Among 403 patients with symptom onset within 30 days, CAS, PAD, and RAS occurrence rates were 68.7%, 25.3%, and 9.9%, respectively. PAD was independently associated with the degree of extracranial and intracranial CAS (p = 0.042, OR = 1.428, 95% CI 1.014-2.012; p = 0.002, OR = 1.680, 95% CI 1.206-2.339), while RAS was independently associated with the degree of extracranial CAS (p = 0.001, OR = 2.880, 95% CI 1.556-5.329). Independent CPAS risk factors included an ischemic stroke history (p = 0.033), increased age (p < 0.01), as well as elevated fibrinogen (p = 0.021) and D-dimer levels (p = 0.019). In conclusion, the occurrence rates of RAS and PAD in ICVD patients with AS is relatively high, and with the severity of RAS or PAD increase, the severity of CAS also increase. Strengthening the evaluation of peripheral AS and controlling elevated fibrinogen might be crucial for preventing and delaying the progression of multiterritorial AS in ICVD patients with AS, thereby improving risk stratification and promoting more effective prevention and treatment strategies.
患有缺血性脑血管病 (ICVD) 的患者常并发外周动脉疾病 (PAD) 或肾动脉狭窄 (RAS),多部位动脉粥样硬化患者的预后通常较差。本研究旨在评估伴有动脉粥样硬化 (AS) 的 ICVD 患者外周动脉粥样硬化 (AS) 和颈颅 AS (CAS) 的现状,及其相关性,以及导致共存颈颅-外周 AS (CPAS) 的相关危险因素。根据 CT 血管造影和超声评估的 AS 严重程度和程度,将 AS 程度三重分类以评估 CAS 与 PAD/RAS 之间的相关性。CAS 和 PAD/RAS 定义为颈颅或下肢动脉管腔狭窄≥50%的最严重狭窄,肾动脉湍流部位的收缩期峰值速度≥180cm/s。在 403 例症状发作在 30 天内的患者中,CAS、PAD 和 RAS 的发生率分别为 68.7%、25.3%和 9.9%。PAD 与颅外和颅内 CAS 的严重程度独立相关(p=0.042,OR=1.428,95%CI 1.014-2.012;p=0.002,OR=1.680,95%CI 1.206-2.339),而 RAS 与颅外 CAS 的严重程度独立相关(p=0.001,OR=2.880,95%CI 1.556-5.329)。独立的 CPAS 危险因素包括缺血性脑卒中病史(p=0.033)、年龄增加(p<0.01)、纤维蛋白原升高(p=0.021)和 D-二聚体水平升高(p=0.019)。总之,AS 合并 ICVD 患者的 RAS 和 PAD 发生率相对较高,随着 RAS 或 PAD 严重程度的增加,CAS 的严重程度也随之增加。加强外周 AS 的评估和控制纤维蛋白原升高可能对预防和延缓 AS 多部位进展至关重要,从而改善风险分层并促进更有效的预防和治疗策略。