Department of Surgery, West Virginia University, Charleston, WV.
Department of Surgery, West Virginia University, Charleston, WV.
J Vasc Surg. 2020 Mar;71(3):937-945. doi: 10.1016/j.jvs.2019.05.050. Epub 2019 Aug 27.
The ankle-brachial index (ABI) may underestimate the severity of peripheral arterial disease (PAD) in patients with noncompressible vessels. This study analyzed limitations of the ABI and toe-brachial index (TBI), if done alone, in patients with symptomatic PAD, diagnosed by duplex ultrasound (DUS) examination, particularly in patients with diabetes and chronic kidney disease (CKD).
This is a retrospective review of prospectively collected data. All patients underwent resting ABIs, TBI, and/or DUS. An ABIs of 0.90 or less in either leg was considered abnormal, and the term inconclusive ABIs (noncompressibility) was used if the ABI was 1.3 or greater. The sensitivity, specificity, positive predictive value, negative predictive value, and overall accuracy (OA) of ABIs in detecting 50% or greater stenosis of any arterial segment based on DUS were determined. A TBI of less than 0.7 was considered abnormal.
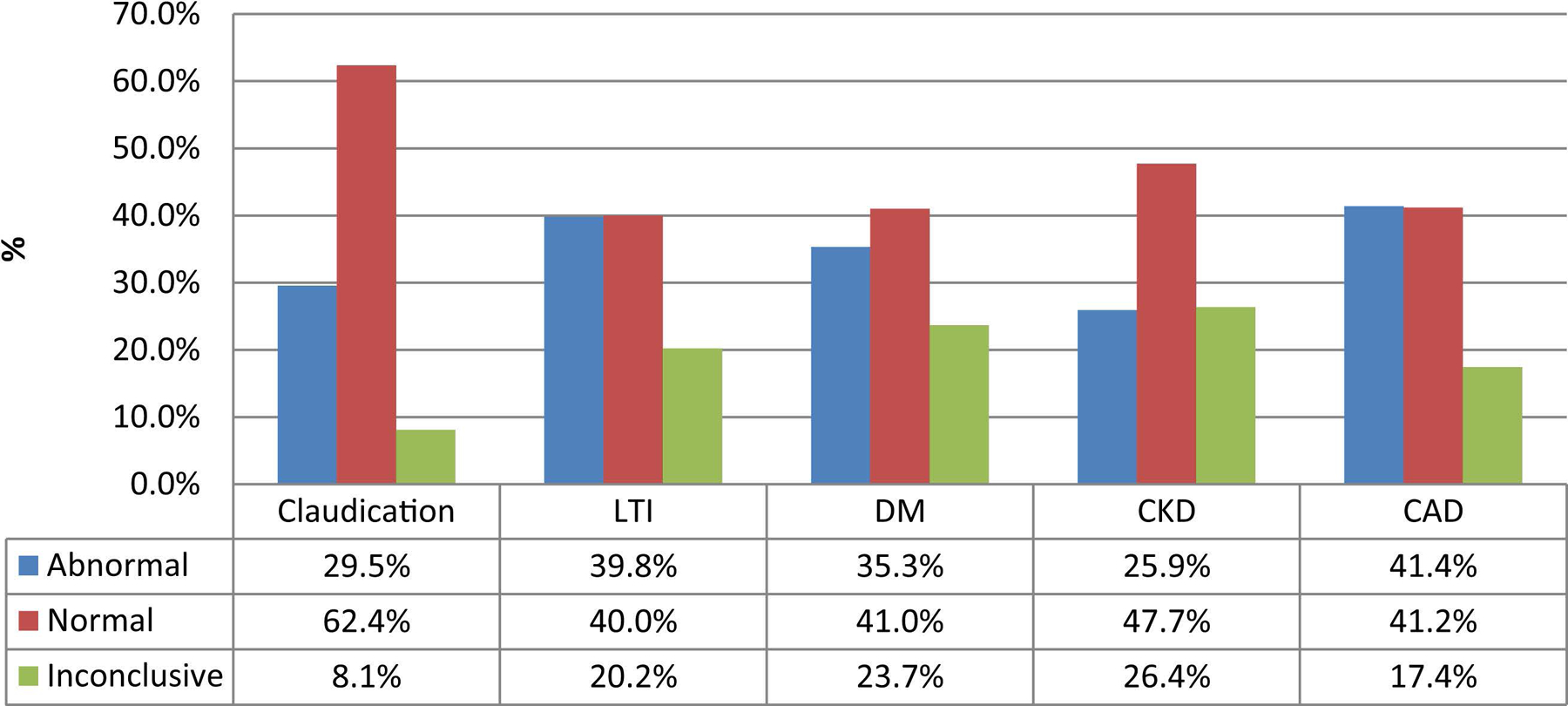
We included 2226 ABIs and 1383 DUS examinations: 46% of patients had diabetes, 16% had CKD, and 39% had coronary artery disease. Fifty-three percent of the ABIs were normal, 34% were abnormal, and 13% were inconclusive. For patients with limb-threatening ischemia, 40% had normal ABIs, 40% abnormal ABIs, and 20% were inconclusive. The sensitivity and OA for ABIs in detecting 50% or greater stenosis in the whole series were 57% (95% confidence interval [CI], 53.7-61.2) and 74% (95% CI, 71.9-76.6); for diabetics 51% (95% CI, 46.1-56.3) and 66% (95% CI, 62.3-69.8); nondiabetics 66% (95% CI, 59.9-70.9) and 81% (95% CI, 78.2-83.9). For patients with CKD, the sensitivity and OA for ABIs in detecting 50% or greater stenosis was 43% (95% CI, 34.3-52.7) and 67% (95% CI, 60.2-73.0) versus patients with no CKD 60% (95% CI, 56.3-64.6) and 76% (95% CI, 73.1-78.1). If patients with inconclusive ABIs were excluded, these values were 69% (95% CI, 65.2-72.9) and 80% (95% CI, 77.2-81.9) in the whole series; 67% (95% CI, 61.6-72.7) and 75% (95% CI, 70.5-78.4) for diabetics; and 63% (95% CI, 51.3-73.0) and 78% (95% CI, 70.6-83.9) for patients with CKD. Thirty-three percent of TBIs were normal and 67% were abnormal. The sensitivity and OA for abnormal TBI in detecting 50% or greater stenosis were 85% (95% CI, 78.9-90.0) and 75% (95% CI, 70.1-80.2) in the whole series; 84% (95% CI, 76.0-90.3) and 74% (95% CI, 67.1-80.2) for diabetics; and 77% (95% CI, 61.4-88.2) and 72% (95% CI, 59.9-82.3) for patients with CKD. For those with inconclusive ABIs, these values for TBI were 75% and 69%.
Of symptomatic patients with PAD with 50% or greater stenosis on DUS examination, 43% had normal/inconclusive resting ABIs (49% in diabetics and 57% in CKD). TBI may help in patients with inconclusive ABIs. These patients should undergo further imaging to determine proper treatment.
踝臂指数(ABI)可能低估了经双功能超声检查(DUS)诊断的有症状外周动脉疾病(PAD)患者的严重程度,尤其在患有非压缩性血管疾病、糖尿病和慢性肾病(CKD)的患者中。本研究分析了在这些患者中,ABI 和趾臂指数(TBI)单独使用的局限性。
这是一项前瞻性数据回顾性研究。所有患者均行静息ABI、TBI 和/或 DUS 检查。ABI 低于 0.90 被认为异常,如果 ABI 为 1.3 或更高,则称为不确定 ABI(非压缩性)。根据 DUS 检查,确定了 ABI 检测任何动脉节段 50%或更大狭窄的灵敏度、特异性、阳性预测值、阴性预测值和总体准确性(OA)。TBI 小于 0.7 被认为异常。
共纳入 2226 例 ABI 和 1383 例 DUS 检查:46%的患者患有糖尿病,16%的患者患有 CKD,39%的患者患有冠心病。53%的 ABI 正常,34%异常,13%不确定。在有肢体缺血危险的患者中,40%的 ABI 正常,40%的 ABI 异常,20%的 ABI 不确定。ABI 检测整个系列中 50%或更大狭窄的灵敏度和 OA 分别为 57%(95%置信区间[CI],53.7-61.2)和 74%(95% CI,71.9-76.6);对于糖尿病患者为 51%(95% CI,46.1-56.3)和 66%(95% CI,62.3-69.8);非糖尿病患者为 66%(95% CI,59.9-70.9)和 81%(95% CI,78.2-83.9)。对于 CKD 患者,ABI 检测 50%或更大狭窄的灵敏度和 OA 分别为 43%(95% CI,34.3-52.7)和 67%(95% CI,60.2-73.0),而非 CKD 患者为 60%(95% CI,56.3-64.6)和 76%(95% CI,73.1-78.1)。如果排除不确定的 ABI,这些值在整个系列中为 69%(95% CI,65.2-72.9)和 80%(95% CI,77.2-81.9);对于糖尿病患者为 67%(95% CI,61.6-72.7)和 75%(95% CI,70.5-78.4);对于 CKD 患者为 63%(95% CI,51.3-73.0)和 78%(95% CI,70.6-83.9)。33%的 TBI 正常,67%异常。ABI 异常检测 50%或更大狭窄的灵敏度和 OA 分别为 85%(95% CI,78.9-90.0)和 75%(95% CI,70.1-80.2),在整个系列中;对于糖尿病患者为 84%(95% CI,76.0-90.3)和 74%(95% CI,67.1-80.2);对于 CKD 患者为 77%(95% CI,61.4-88.2)和 72%(95% CI,59.9-82.3)。对于不确定的 ABI,这些值为 TBI 的 75%和 69%。
在经 DUS 检查诊断为有症状 PAD 且狭窄程度为 50%或更大的患者中,43%的患者静息ABI 正常/不确定(糖尿病患者为 49%,CKD 患者为 57%)。TBI 可能有助于不确定 ABI 的患者。这些患者应进一步进行影像学检查以确定适当的治疗方法。