Translational Neuroimmunology Group, Kids Neuroscience Centre and Sydney Medical School, Faculty of Medicine and Health, University of Sydney, Sydney, NSW, Australia.
Department of Neurology, Westmead Hospital, Sydney, NSW, Australia.
Eye (Lond). 2024 Aug;38(12):2289-2301. doi: 10.1038/s41433-024-03108-y. Epub 2024 May 23.
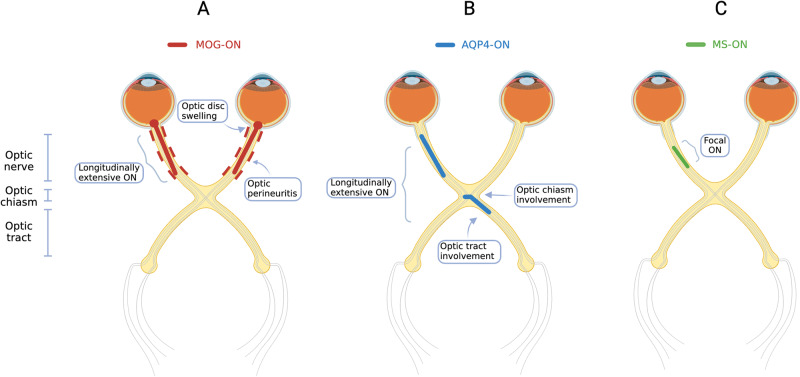
Myelin oligodendrocyte glycoprotein (MOG) antibody-associated disease (MOGAD) is a demyelinating disorder, distinct from multiple sclerosis (MS) and neuromyelitis optica spectrum disorder (NMOSD). MOGAD most frequently presents with optic neuritis (MOG-ON), often with characteristic clinical and radiological features. Bilateral involvement, disc swelling clinically and radiologically, and longitudinally extensive optic nerve hyperintensity with associated optic perineuritis on MRI are key characteristics that can help distinguish MOG-ON from optic neuritis due to other aetiologies. The detection of serum MOG immunoglobulin G utilising a live cell-based assay in a patient with a compatible clinical phenotype is highly specific for the diagnosis of MOGAD. This review will highlight the key clinical and radiological features which expedite diagnosis, as well as ancillary investigations such as visual fields, visual evoked potentials and cerebrospinal fluid analysis, which may be less discriminatory. Optical coherence tomography can identify optic nerve swelling acutely, and atrophy chronically, and may transpire to have utility as a diagnostic and prognostic biomarker. MOG-ON appears to be largely responsive to corticosteroids, which are often the mainstay of acute management. However, relapses are common in patients in whom follow-up is prolonged, often in the context of early or rapid corticosteroid tapering. Establishing optimal acute therapy, the role of maintenance steroid-sparing immunotherapy for long-term relapse prevention, and identifying predictors of relapsing disease remain key research priorities in MOG-ON.
髓鞘少突胶质细胞糖蛋白 (MOG) 抗体相关性疾病 (MOGAD) 是一种脱髓鞘疾病,与多发性硬化症 (MS) 和视神经脊髓炎谱系障碍 (NMOSD) 不同。MOGAD 最常表现为视神经炎 (MOG-ON),常具有特征性的临床和影像学特征。双侧受累、临床和影像学上的盘肿胀、以及与视神经周围炎相关的长节段视神经强化,是有助于将 MOG-ON 与其他病因引起的视神经炎相区分的关键特征。在具有相容临床表型的患者中,利用活细胞检测试剂盒检测血清 MOG 免疫球蛋白 G 对于 MOGAD 的诊断具有高度特异性。这篇综述将重点介绍有助于快速诊断的关键临床和影像学特征,以及辅助检查,如视野、视觉诱发电位和脑脊液分析,这些检查的鉴别能力可能较低。光学相干断层扫描可以在急性时识别视神经肿胀,在慢性时识别视神经萎缩,并且可能作为一种诊断和预后生物标志物具有一定的应用价值。MOG-ON 似乎对皮质类固醇反应良好,皮质类固醇通常是急性治疗的主要方法。然而,在随访时间延长的患者中,复发很常见,尤其是在早期或快速减少皮质类固醇的情况下。确定最佳急性治疗方案、维持类固醇免疫抑制治疗以预防长期复发的作用,以及识别复发性疾病的预测因素,仍然是 MOG-ON 研究的重点。