Doshi Mona D, Li Lihua, Naik Abhijit S, Thomas Christie P
Division of Nephrology, Department of Medicine, University of Michigan, Ann Arbor, MI.
Department of Population Health Science and Policy, Icahn School of Medicine at Mount Sinai, New York, NY.
Kidney Med. 2024 Apr 17;6(6):100828. doi: 10.1016/j.xkme.2024.100828. eCollection 2024 Jun.
RATIONALE & OBJECTIVE: The effect of apolipoprotein L1( genotype on future risk of kidney disease among middle-aged individuals with good kidney function is not well established.
Longitudinal cohort study.
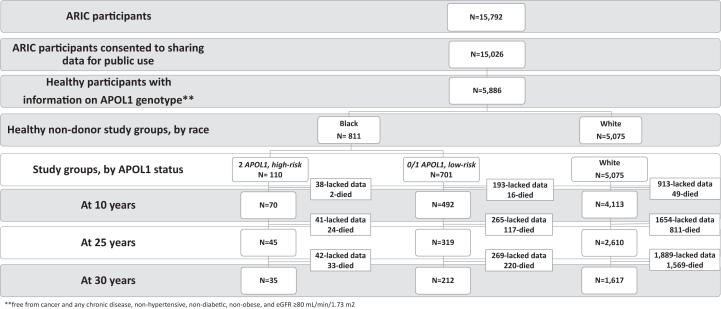
SETTING & PARTICIPANTS: In total, 5,886 healthy individuals (45-64 years old) enrolled in the Atherosclerosis Risk in Communities study with creatinine-based estimated glomerular filtration rate ≥ 80 mL/min who would be suitable kidney donors.
Race and genotype.
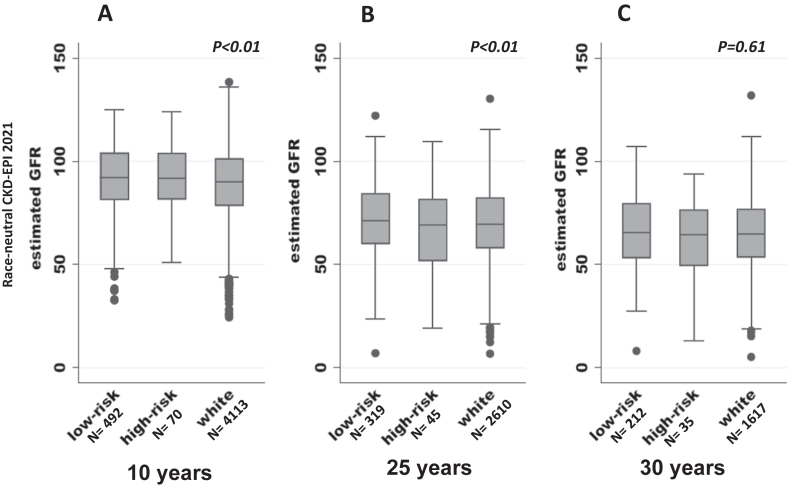
Creatinine- and cystatin C-based estimated glomerular filtration rate (eGFRcr-cys) using the CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) 2021 equation, urinary albumin-creatinine ratio (UACR), proportion with chronic kidney disease (CKD) 3a or worse, end-stage kidney disease (ESKD), and death.
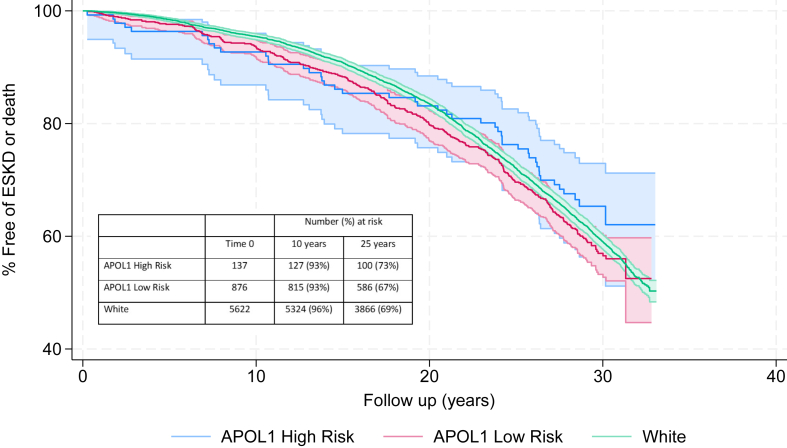
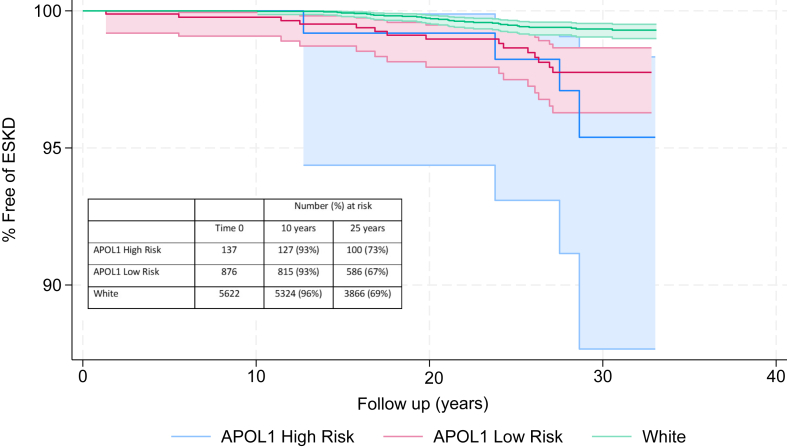
Participants grouped based on race and genotype. Compared eGFRcr-cys and UACR across groups. Multinomial logistic regression models were used compare odds of CKD. Kaplan-Meier survival curves were created to compare rates of ESKD and death at last follow-up.
There were 5,075 Whites (86%), 701 Blacks carrying the low-risk genotype (12%), and 110 Blacks carrying the high-risk A genotype (2%). The mean age at baseline was 53 ± 6 years. At 10 years, White participants had lower eGFRcr-cys than low-risk and high-risk groups (89 ± 16 vs 91 ± 16 and 92 ± 15 mL/min/1.73 m, respectively; < 0.001). At 25 years, White participants continued to have lower eGFRcr-cys than the low-risk group (70 ± 18 vs 72 ± 19 mL/min/1.73 m; < 0.001) but not compared with the high-risk genotype (67±23 mL/min/1.73 m). There was no difference in UACR among groups at 10 and 25 years ( = 0.87 and 0.91, respectively). The odds of developing CKD stage 3a or worse were not different between low-risk and high-risk group in both unadjusted and adjusted models ( = 0.26 and = 0.39, respectively). At last follow-up, <5% developed ESKD, and 45% of individuals either died or reached ESKD with no difference in outcomes between the groups.
Low ascertainment because of death and long follow-up.
Among middle-aged individuals, genotype does not appear to be a major driver of future risk of kidney disease.
载脂蛋白L1(APOL1)基因型对肾功能良好的中年个体未来患肾病风险的影响尚未明确。
纵向队列研究。
共有5886名健康个体(45 - 64岁)参与社区动脉粥样硬化风险研究,其基于肌酐的估计肾小球滤过率≥80 mL/min,适合作为肾脏供体。
种族和APOL1基因型。
使用慢性肾脏病流行病学协作组(CKD - EPI)2021方程基于肌酐和胱抑素C的估计肾小球滤过率(eGFRcr - cys)、尿白蛋白肌酐比值(UACR)、慢性肾脏病(CKD)3a期或更严重阶段的比例、终末期肾病(ESKD)以及死亡情况。
参与者根据种族和APOL1基因型分组。比较各组间的eGFRcr - cys和UACR。使用多项逻辑回归模型比较CKD的发病几率。绘制Kaplan - Meier生存曲线以比较最后一次随访时ESKD和死亡的发生率。
有5075名白人(86%),701名携带低风险APOL1基因型的黑人(12%),以及110名携带高风险A基因型的黑人(2%)。基线时的平均年龄为53±6岁。10年后,白人参与者的eGFRcr - cys低于低风险和高风险组(分别为89±16 vs 91±16和92±15 mL/min/1.73m²;P<0.001)。25年后,白人参与者的eGFRcr - cys继续低于低风险组(70±18 vs 72±19 mL/min/1.73m²;P<0.001),但与高风险APOL1基因型组相比无差异(67±23 mL/min/1.73m²)。10年和25年时各组间UACR无差异(分别为P = 0.87和P = 0.91)。在未调整和调整模型中,低风险和高风险APOL1基因型组发生CKD 3a期或更严重阶段的几率无差异(分别为P = 0.26和P = 0.39)。在最后一次随访时,<5%的人发展为ESKD,45%的个体死亡或达到ESKD,各组间结局无差异。
由于死亡和随访时间长导致确诊率低(确定率低)。
在中年个体中,APOL1基因型似乎不是未来患肾病风险的主要驱动因素。