Department of Medicine, Icahn School of Medicine at Mount Sinai, New York, NY, USA.
Department of Medicine, Montefiore Medical Center, Bronx, NY, USA.
BMC Cardiovasc Disord. 2024 May 30;24(1):283. doi: 10.1186/s12872-024-03962-4.
BACKGROUND & OBJECTIVE: Despite their continued use, the effectiveness and safety of vasopressors in post-cardiac arrest patients remain controversial. This study examined the efficacy of various vasopressors in cardiac arrest patients in terms of clinical, morbidity, and mortality outcomes.
A comprehensive literature search was performed using online databases (MeSH terms: MEDLINE (Ovid), CENTRAL (Cochrane Library), Embase (Ovid), CINAHL, Scopus, and Google Scholar) from 1997 to 2023 for relevant English language studies. The primary outcomes of interest for this study included short-term survival leading to death, return of spontaneous circulation (ROSC), survival to hospital discharge, neurological outcomes, survival to hospital admission, myocardial infarction, and incidence of arrhythmias.
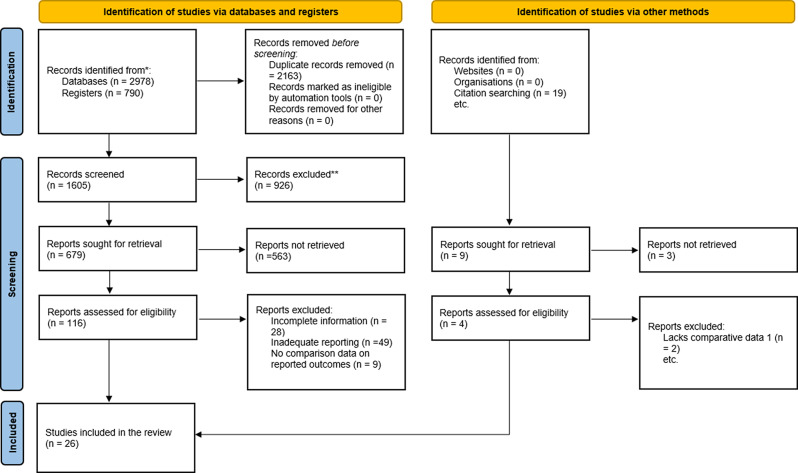
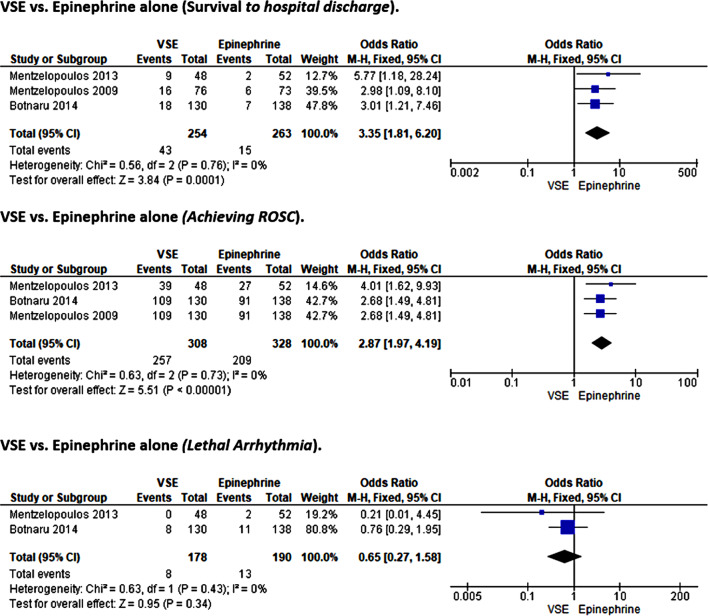
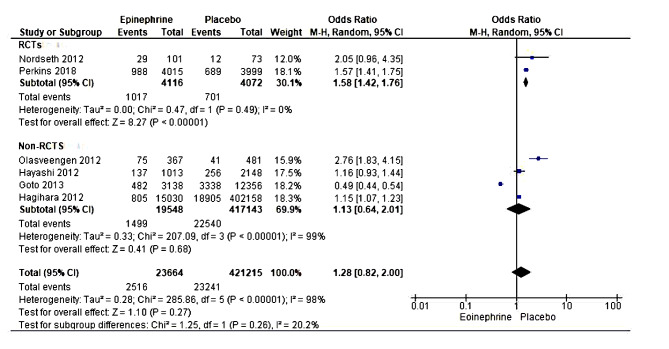
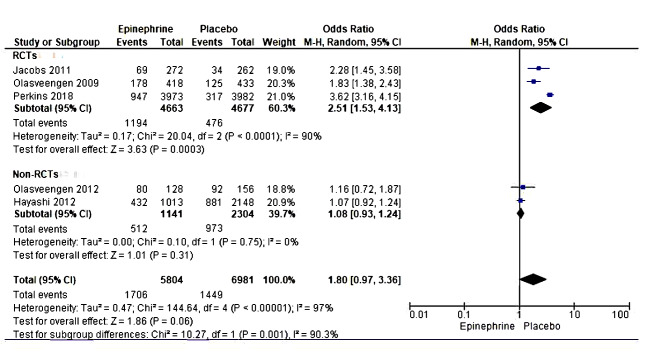
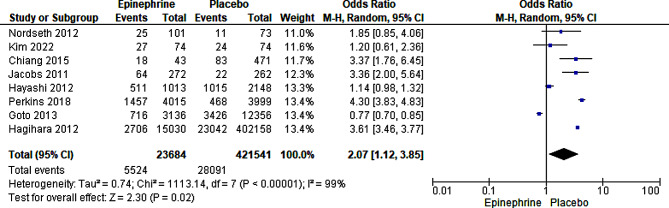
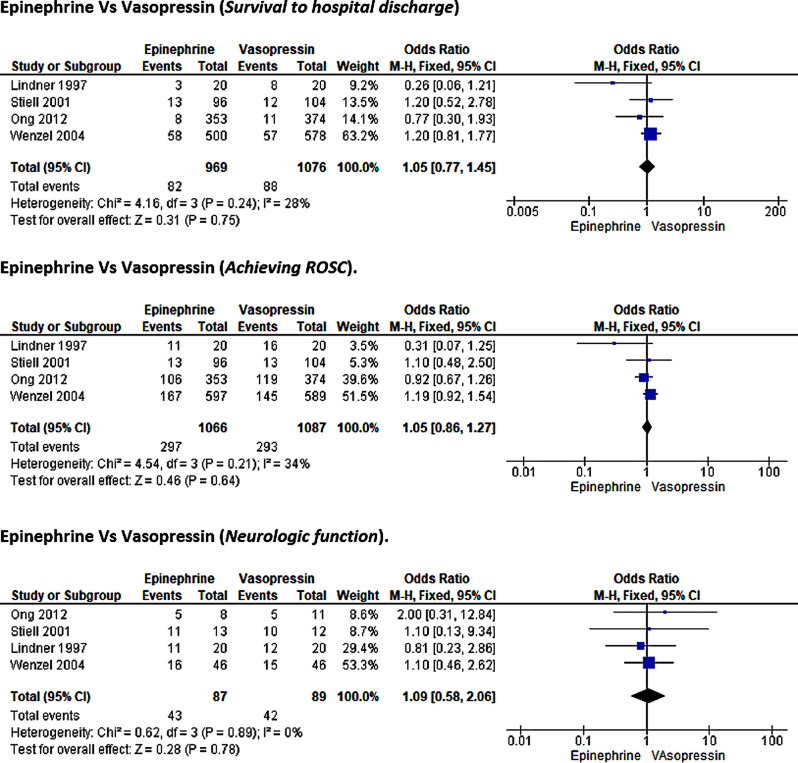
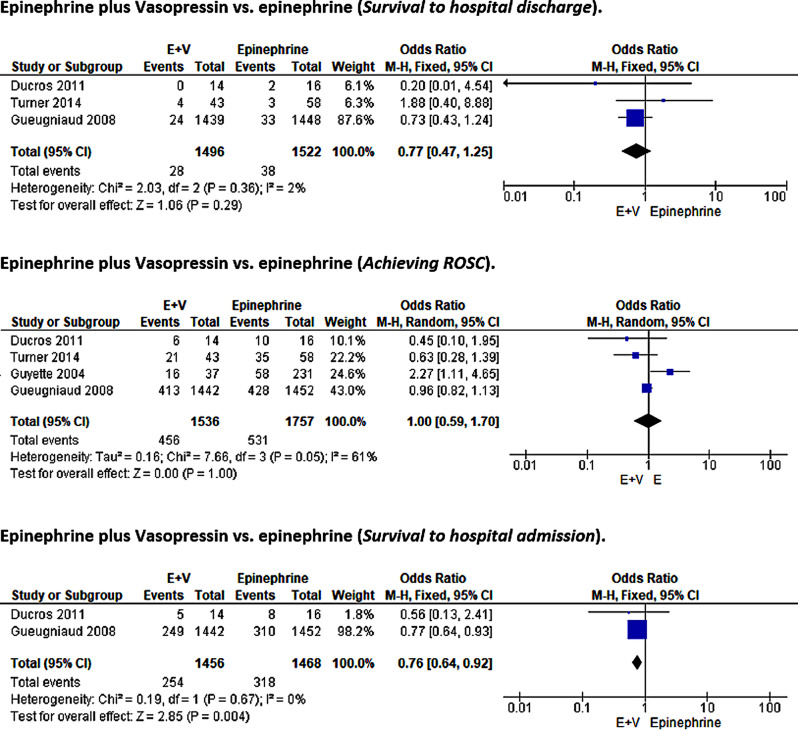
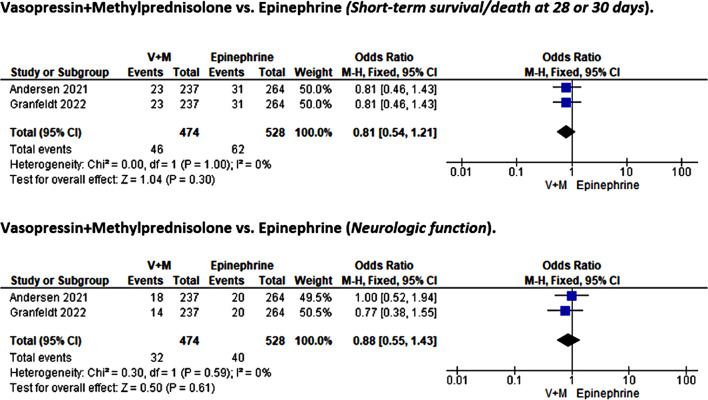
In this meta-analysis, 26 studies, including 16 RCTs and ten non-RCTs, were evaluated. The focus was on the efficacy of epinephrine, vasopressin, methylprednisolone, dopamine, and their combinations in medical emergencies. Epinephrine treatment was associated with better odds of survival to hospital discharge (OR = 1.52, 95%CI [1.20, 1.94]; p < 0.001) and achieving ROSC (OR = 3.60, 95% CI [3.45, 3.76], P < 0.00001)) over placebo but not in other outcomes of interest such as short-term survival/ death at 28-30 days, survival to hospital admission, or neurological function. In addition, our analysis indicates non-superiority of vasopressin or epinephrine vasopressin-plus-epinephrine therapy over epinephrine monotherapy except for survival to hospital admission where the combinatorial therapy was associated with better outcome (0.76, 95%CI [0.64, 0.92]; p = 0.004). Similarly, we noted the non-superiority of vasopressin-plus-methylprednisolone versus placebo. Finally, while higher odds of survival to hospital discharge (OR = 3.35, 95%CI [1.81, 6.2]; p < 0.001) and ROSC (OR = 2.87, 95%CI [1.97, 4.19]; p < 0.001) favoring placebo over VSE therapy were observed, the risk of lethal arrhythmia was not statistically significant. There was insufficient literature to assess the effects of dopamine versus other treatment modalities meta-analytically.
This meta-analysis indicated that only epinephrine yielded superior outcomes among vasopressors than placebo, albeit limited to survival to hospital discharge and ROSC. Additionally, we demonstrate the non-superiority of vasopressin over epinephrine, although vasopressin could not be compared to placebo due to the paucity of data. The addition of vasopressin to epinephrine treatment only improved survival to hospital admission.
尽管血管加压素仍在继续使用,但在心脏骤停患者中的有效性和安全性仍存在争议。本研究旨在从临床、发病率和死亡率等方面评估心脏骤停患者中各种血管加压素的疗效。
通过在线数据库(MeSH 术语:MEDLINE(Ovid)、CENTRAL(Cochrane 图书馆)、Embase(Ovid)、CINAHL、Scopus 和 Google Scholar),对 1997 年至 2023 年的相关英文文献进行全面文献检索。本研究的主要结局包括短期存活至死亡、自主循环恢复(ROSC)、存活至出院、神经功能结局、存活至入院、心肌梗死和心律失常发生率。
本荟萃分析共纳入 26 项研究,包括 16 项 RCT 和 10 项非 RCT。重点评估了肾上腺素、血管加压素、甲泼尼龙、多巴胺及其组合在医疗急救中的疗效。与安慰剂相比,肾上腺素治疗与更高的出院存活率(OR=1.52,95%CI [1.20,1.94];p<0.001)和实现 ROSC(OR=3.60,95%CI [3.45,3.76],P<0.00001)相关,但与其他感兴趣的结局(如 28-30 天的短期存活/死亡、存活至入院或神经功能)无关。此外,我们的分析表明,血管加压素或肾上腺素血管加压素加肾上腺素治疗并不优于肾上腺素单药治疗,除了入院存活率外,联合治疗与更好的结局相关(0.76,95%CI [0.64,0.92];p=0.004)。同样,我们注意到血管加压素加甲泼尼龙与安慰剂相比无优势。最后,尽管观察到安慰剂优于 VSE 治疗的更高出院存活率(OR=3.35,95%CI [1.81,6.2];p<0.001)和 ROSC(OR=2.87,95%CI [1.97,4.19];p<0.001),但致命性心律失常的风险并无统计学意义。由于文献不足,无法进行多巴胺与其他治疗方式的荟萃分析来评估其效果。
本荟萃分析表明,只有肾上腺素在血管加压素中比安慰剂产生更好的结果,尽管仅限于出院存活率和 ROSC。此外,我们证明了血管加压素不如肾上腺素优越,尽管由于数据不足,无法将血管加压素与安慰剂进行比较。血管加压素加肾上腺素治疗仅改善了入院存活率。