Health Services Research Unit, University of Aberdeen, Aberdeen, AB25 2ZD, Scotland, UK.
School of Divinity, History, Philosophy and Art History, University of Aberdeen, Aberdeen, Scotland, UK.
BMC Prim Care. 2024 May 31;25(1):193. doi: 10.1186/s12875-024-02443-z.
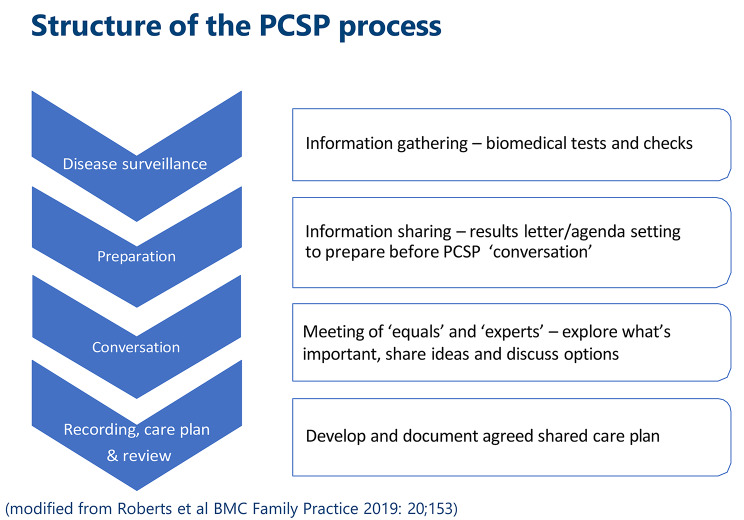
Personalised Care and Support Planning (PCSP) replaces conventional annual reviews for people with long-term conditions. It is designed to help healthcare professionals (HCPs) and patients engage in conversations as equals and collaboratively plan actions oriented to each patient's priorities, alongside biomedical concerns. Little is known about how the shift to remote consulting initiated with COVID-19 restrictions has impacted PCSP.
To investigate HCPs' experiences of conducting PCSP conversations remotely and consider implications for the fulfilment of PCSP ambitions as remote consulting continues beyond COVID-19 restrictions.
19 semi-structured interviews with HCPs in England and Scotland; interpretive analysis.
HCPs' accounts made clear that COVID-19 restrictions impacted multiple aspects of PCSP delivery, not just the mode of conversation. Broader disruption to general practice systems for gathering and sharing information ahead of PCSP conversations, and moves to 'wide window' appointment times, made it harder for patients to be prepared for PCSP conversations. This constrained scope to achieve PCSP ambitions even with the best professional communication skills. Most remote PCSP conversations were conducted by telephone. In the absence of visual communication with patients, it was sometimes harder to achieve the ambitions of PCSP conversations, including to balance patient and professional agendas, fulfil key planning activities, and foster a relational ethos of equal, collaborative partnership. The challenges were particularly severe when working with new patients and people with complex clinical and social problems. Although options for telephone appointments now offer valued flexibility, sustained experience of struggling to achieve PCSP ambitions via remote consulting led some HCPs to lower their standards for judging a "good" PCSP conversation, and to diminished professional satisfaction.
There are significant challenges to fulfilling the ambitions of PCSP via telephone, especially when preparatory support is limited. This study provides grounds for scepticism about how compatible telephone appointments can be with this person-centred model of working, especially for people who are socially disadvantaged and live with complex health conditions. These threats to the provision of person-centred support for people with long-term conditions warrant careful attention going forward if the PCSP model and its benefits are to be sustained.
个性化护理和支持计划(PCSP)取代了长期疾病患者的常规年度评估。它旨在帮助医疗保健专业人员(HCP)和患者进行平等对话,并共同规划针对每位患者优先事项和生物医学问题的行动。对于 COVID-19 限制引发的远程咨询对 PCSP 的影响知之甚少。
调查 HCP 远程进行 PCSP 对话的经验,并考虑在 COVID-19 限制结束后继续远程咨询的情况下,实现 PCSP 目标的影响。
对英格兰和苏格兰的 19 名 HCP 进行半结构化访谈;解释性分析。
HCP 的描述清楚地表明,COVID-19 限制不仅影响了 PCSP 交付的模式,还影响了多个方面。在 PCSP 对话之前收集和共享信息的一般实践系统更广泛的中断,以及向“宽窗口”预约时间的转变,使得患者更难为 PCSP 对话做好准备。即使拥有最佳的专业沟通技巧,也限制了实现 PCSP 目标的范围。大多数远程 PCSP 对话都是通过电话进行的。在没有与患者进行视觉交流的情况下,有时更难实现 PCSP 对话的目标,包括平衡患者和专业人员的议程、完成关键的规划活动,并培养平等、合作伙伴关系的关系伦理。当与新患者和患有复杂临床和社会问题的患者合作时,这些挑战尤其严重。尽管现在有电话预约的选择提供了有价值的灵活性,但通过远程咨询努力实现 PCSP 目标的持续经验导致一些 HCP 降低了判断“良好”PCSP 对话的标准,并降低了职业满意度。
通过电话实现 PCSP 的目标存在重大挑战,特别是在预备支持有限的情况下。这项研究对电话预约与这种以患者为中心的工作模式的兼容性提出了质疑,特别是对于那些社会劣势和患有复杂健康状况的人。如果要维持 PCSP 模式及其益处,就需要对长期疾病患者提供以患者为中心的支持的威胁给予谨慎关注。