Cancer Behavioural Science Cancer Prevention Group, King's College, London, UK.
Professor of Health Psychology, Queen Mary University London, London, UK.
Med Decis Making. 2024 Jul;44(5):586-600. doi: 10.1177/0272989X241254828. Epub 2024 Jun 3.
A risk-stratified breast screening program could offer low-risk women less screening than is currently offered by the National Health Service. The acceptability of this approach may be enhanced if it corresponds to UK women's screening preferences and values.
To elicit and quantify preferences for low-risk screening options.
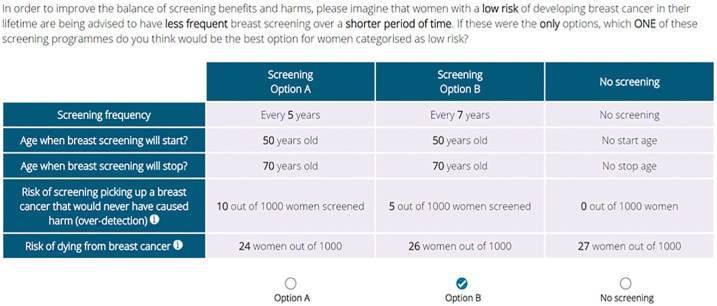
Women aged 40 to 70 y with no history of breast cancer took part in an online discrete choice experiment. We generated 32 hypothetical low-risk screening programs defined by 5 attributes (start age, end age, screening interval, risk of dying from breast cancer, and risk of overdiagnosis), the levels of which were systematically varied between the programs. Respondents were presented with 8 choice sets and asked to choose between 2 screening alternatives or no screening. Preference data were analyzed using conditional logit regression models. The relative importance of attributes and the mean predicted probability of choosing each program were estimated.
Participants ( = 502) preferred all screening programs over no screening. An older starting age of screening, younger end age of screening, longer intervals between screening, and increased risk of dying had a negative impact on support for screening programs ( < 0.01). Although the risk of overdiagnosis was of low relative importance, a decreased risk of this harm had a small positive impact on screening choices. The mean predicted probabilities that risk-adapted screening programs would be supported relative to current guidelines were low (range, 0.18 to 0.52).
A deintensified screening pathway for women at low risk of breast cancer, especially one that recommends a later screening start age, would run counter to women's breast screening preferences. Further research is needed to enhance the acceptability of offering less screening to those at low risk of breast cancer.
Risk-based breast screening may involve the deintensification of screening for women at low risk of breast cancer.Low-risk screening pathways run counter to women's screening preferences and values.Longer screening intervals may be preferable to a later start age.Work is needed to enhance the acceptability of a low-risk screening pathway.
风险分层的乳房筛查计划可能会为低风险女性提供比国民保健服务目前提供的更少的筛查。如果这种方法符合英国女性的筛查偏好和价值观,那么这种方法的可接受性可能会提高。
确定并量化对低风险筛查方案的偏好。
40 至 70 岁之间没有乳腺癌病史的女性参加了在线离散选择实验。我们生成了 32 个假设的低风险筛查计划,由 5 个属性(起始年龄、结束年龄、筛查间隔、死于乳腺癌的风险和过度诊断的风险)定义,这些属性在计划之间系统地变化。受访者被提供了 8 个选择集,并被要求在 2 个筛查选择或不筛查之间进行选择。使用条件逻辑回归模型分析偏好数据。估计属性的相对重要性和选择每个方案的平均预测概率。
参与者( = 502)更喜欢所有筛查计划而不是不筛查。筛查年龄较大、筛查年龄较年轻、筛查间隔较长以及死于乳腺癌的风险增加对支持筛查计划产生了负面影响( < 0.01)。尽管过度诊断的风险相对不重要,但这种危害的风险降低对筛查选择有较小的积极影响。与现行指南相比,风险适应性筛查计划得到支持的平均预测概率较低(范围为 0.18 至 0.52)。
对于低乳腺癌风险的女性,一种去强化的乳腺癌筛查途径,特别是建议推迟筛查起始年龄的途径,可能与女性的乳房筛查偏好背道而驰。需要进一步研究以提高对低乳腺癌风险女性提供较少筛查的可接受性。
基于风险的乳房筛查可能涉及降低低乳腺癌风险女性的筛查强度。低风险的筛查途径与女性的筛查偏好和价值观相悖。较长的筛查间隔可能比较晚的起始年龄更可取。需要做更多的工作来提高低风险筛查途径的可接受性。