Respiratory Diseases Unit, Department of Medical and Surgical Sciences, University Hospital of Modena, University of Modena Reggio Emilia, Modena, Italy.
Laboratory of Cell Therapies and Respiratory Medicine, Department of Medical and Surgical Sciences for Children and Adults, University Hospital of Modena, Modena, Italy.
Sci Rep. 2024 Jun 7;14(1):13158. doi: 10.1038/s41598-024-63670-z.
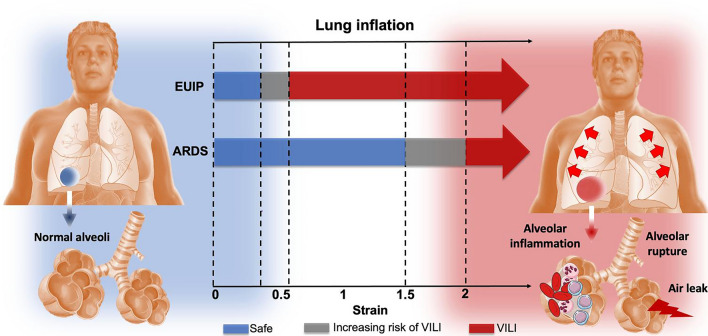
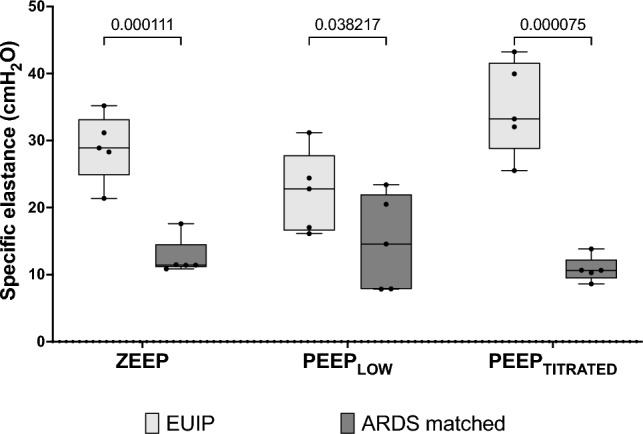
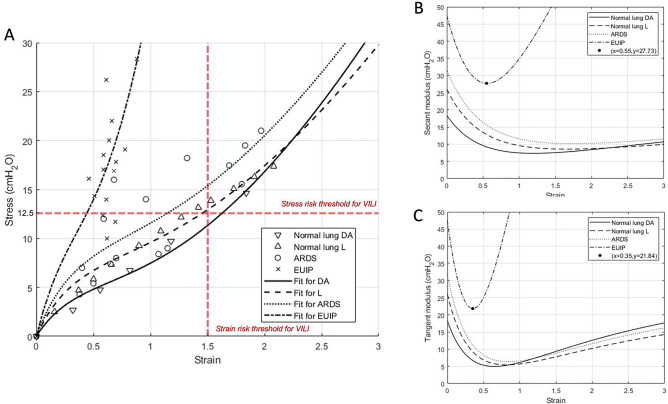
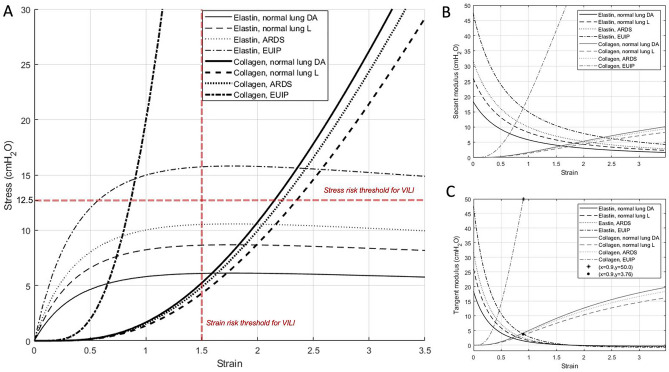
Patients with acute exacerbation of lung fibrosis with usual interstitial pneumonia (EUIP) pattern are at increased risk for ventilator-induced lung injury (VILI) and mortality when exposed to mechanical ventilation (MV). Yet, lack of a mechanical model describing UIP-lung deformation during MV represents a research gap. Aim of this study was to develop a constitutive mathematical model for UIP-lung deformation during lung protective MV based on the stress-strain behavior and the specific elastance of patients with EUIP as compared to that of acute respiratory distress syndrome (ARDS) and healthy lung. Partitioned lung and chest wall mechanics were assessed for patients with EUIP and primary ARDS (1:1 matched based on body mass index and PaO/FiO ratio) during a PEEP trial performed within 24 h from intubation. Patient's stress-strain curve and the lung specific elastance were computed and compared with those of healthy lungs, derived from literature. Respiratory mechanics were used to fit a novel mathematical model of the lung describing mechanical-inflation-induced lung parenchyma deformation, differentiating the contributions of elastin and collagen, the main components of lung extracellular matrix. Five patients with EUIP and 5 matched with primary ARDS were included and analyzed. Global strain was not different at low PEEP between the groups. Overall specific elastance was significantly higher in EUIP as compared to ARDS (28.9 [22.8-33.2] cmHO versus 11.4 [10.3-14.6] cmHO, respectively). Compared to ARDS and healthy lung, the stress/strain curve of EUIP showed a steeper increase, crossing the VILI threshold stress risk for strain values greater than 0.55. The contribution of elastin was prevalent at lower strains, while the contribution of collagen was prevalent at large strains. The stress/strain curve for collagen showed an upward shift passing from ARDS and healthy lungs to EUIP lungs. During MV, patients with EUIP showed different respiratory mechanics, stress-strain curve and specific elastance as compared to ARDS patients and healthy subjects and may experience VILI even when protective MV is applied. According to our mathematical model of lung deformation during mechanical inflation, the elastic response of UIP-lung is peculiar and different from ARDS. Our data suggest that patients with EUIP experience VILI with ventilatory setting that are lung-protective for patients with ARDS.
具有寻常型间质性肺炎(UIP)模式的肺纤维化急性加重患者在接受机械通气(MV)时,发生呼吸机诱导肺损伤(VILI)和死亡的风险增加。然而,缺乏描述 UIP 肺在 MV 期间变形的机械模型是一个研究空白。本研究的目的是基于 UIP 患者的应变-应力行为和特定弹性与急性呼吸窘迫综合征(ARDS)和健康肺的比较,为 UIP 肺在保护性 MV 期间的变形建立一个本构数学模型。对 UIP 患者和原发性 ARDS 患者(根据 BMI 和 PaO/FiO 比值进行 1:1 匹配)在插管后 24 小时内进行的 PEEP 试验中,评估肺和胸壁力学。计算患者的应变-应力曲线和肺特定弹性,并与文献中健康肺的结果进行比较。使用呼吸力学来拟合一种新的描述机械充气诱导肺实质变形的肺数学模型,区分弹性蛋白和胶原蛋白(肺细胞外基质的主要成分)的贡献。共纳入和分析了 5 例 UIP 患者和 5 例原发性 ARDS 患者。两组在低 PEEP 时整体应变没有差异。与 ARDS 相比,UIP 的整体特定弹性明显更高(分别为 28.9[22.8-33.2]cmH2O 和 11.4[10.3-14.6]cmH2O)。与 ARDS 和健康肺相比,UIP 的应变-应力曲线在应变值大于 0.55 时表现出更陡峭的增加,超过了 VILI 风险的阈值应变。在较低的应变时,弹性蛋白的贡献占主导地位,而在较大的应变时,胶原蛋白的贡献占主导地位。胶原的应变-应力曲线从 ARDS 和健康肺转移到 UIP 肺时出现向上移动。在 MV 期间,与 ARDS 患者和健康受试者相比,UIP 患者表现出不同的呼吸力学、应变-应力曲线和特定弹性,即使应用保护性 MV,也可能发生 VILI。根据我们在机械充气过程中肺变形的数学模型,UIP 肺的弹性反应是特殊的,与 ARDS 不同。我们的数据表明,在为 ARDS 患者提供保护性通气的情况下,UIP 患者会发生 VILI。