Heerspink Hiddo J L, Agarwal Rajiv, Bakris George L, Cherney David Z I, Lam Carolyn S P, Neuen Brendon L, Sarafidis Pantelis A, Tuttle Katherine R, Wanner Christoph, Brinker Meike D, Dizayee Sara, Kolkhof Peter, Schloemer Patrick, Vesterinen Paula, Perkovic Vlado
Department of Clinical Pharmacy and Pharmacology, University of Groningen, Groningen, The Netherlands.
Division of Nephrology, Department of Medicine, Indiana University School of Medicine and RL Roudebush VA Medical Center, Indianapolis, IN, USA.
Nephrol Dial Transplant. 2025 Feb 4;40(2):308-319. doi: 10.1093/ndt/gfae132.
Finerenone, a non-steroidal mineralocorticoid receptor antagonist, improved kidney and cardiovascular outcomes in patients with chronic kidney disease (CKD) and type 2 diabetes in two phase 3 outcome trials. The Finerenone, in addition to standard of care, on the progression of kidney disease in patients with Non-Diabetic Chronic Kidney Disease (FIND-CKD) study investigates the effect of finerenone in adults with CKD without diabetes.
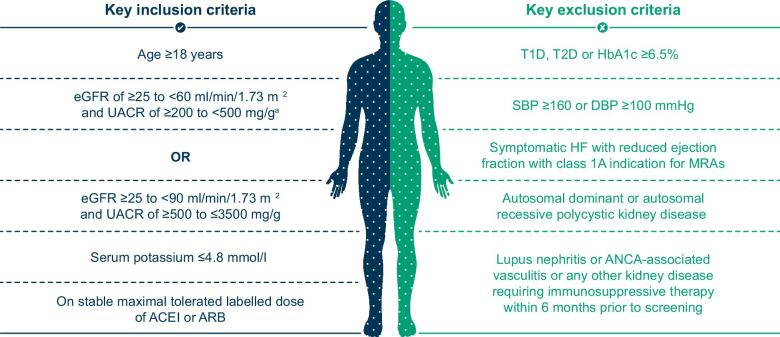
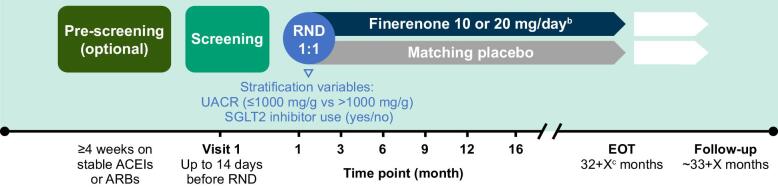
FIND-CKD (NCT05047263 and EU CT 2023-506897-11-00) is a randomized, double-blind, placebo-controlled phase 3 trial in patients with CKD of non-diabetic aetiology. Adults with a urinary albumin:creatinine ratio (UACR) ≥200-≤3500 mg/g and an estimated glomerular filtration rate (eGFR) ≥25-<90 ml/min/1.73 m2 receiving a maximum tolerated dose of a renin-angiotensin system inhibitor were randomized 1:1 to once-daily placebo or finerenone 10 or 20 mg depending on eGFR >60 or <60 ml/min/1.73 m2. The primary efficacy outcome is total eGFR slope, defined as the mean annual rate of change in eGFR from baseline to month 32. Secondary efficacy outcomes include a combined cardiorenal composite outcome comprising time to kidney failure, sustained ≥57% decrease in eGFR, hospitalization for heart failure or cardiovascular death, as well as separate kidney and cardiovascular composite outcomes. Adverse events are recorded to assess tolerability and safety.
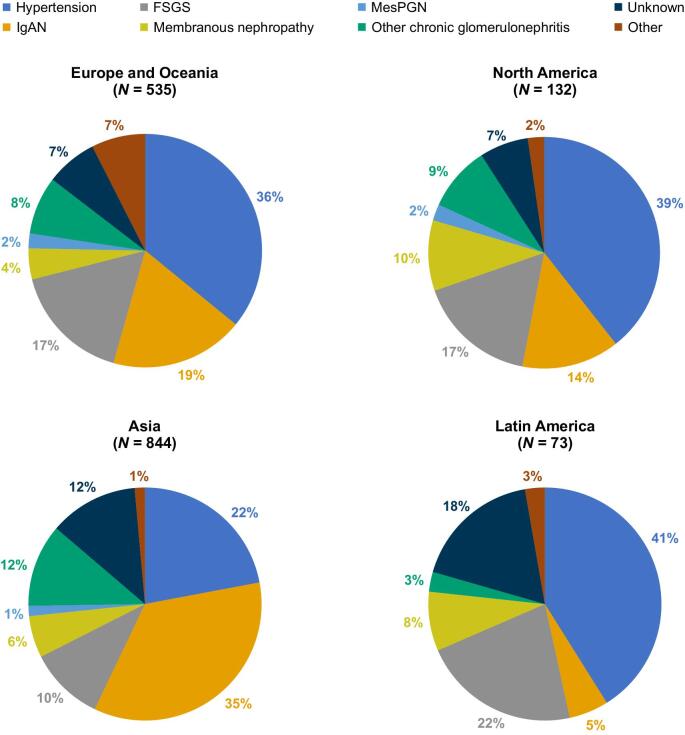
Across 24 countries, 3231 patients were screened and 1584 were randomized to study treatment. The most common causes of CKD were chronic glomerulonephritis (57.0%) and hypertensive/ischaemic nephropathy (29.0%). Immunoglobulin A nephropathy was the most common glomerulonephritis (26.3% of the total population). At baseline, mean eGFR and median UACR were 46.7 ml/min/1.73 m2 and 818.9 mg/g, respectively. Diuretics were used by 282 participants (17.8%), statins by 851 (53.7%) and calcium channel blockers by 794 (50.1%). Sodium-glucose co-transporter 2 (SGLT2) inhibitors were used in 16.9% of patients; these individuals had a similar mean eGFR (45.6 versus 46.8 ml/min/1.73 m2) and a slightly higher median UACR (871.9 versus 808.3 mg/g) compared with those not using SGLT2 inhibitors at baseline.
FIND-CKD is the first phase 3 trial of finerenone in patients with CKD of non-diabetic aetiology.
非甾体类盐皮质激素受体拮抗剂非奈利酮在两项3期试验中改善了慢性肾脏病(CKD)合并2型糖尿病患者的肾脏和心血管结局。非奈利酮治疗非糖尿病慢性肾脏病(FIND-CKD)研究除标准治疗外,还探讨了非奈利酮对无糖尿病的CKD成人患者肾病进展的影响。
FIND-CKD(NCT05047263和欧盟CT 2023-506897-11-00)是一项针对非糖尿病病因的CKD患者的随机、双盲、安慰剂对照3期试验。尿白蛋白与肌酐比值(UACR)≥200至≤3500mg/g且估计肾小球滤过率(eGFR)≥25至<90ml/min/1.73m²并接受最大耐受剂量肾素-血管紧张素系统抑制剂治疗的成年人,根据eGFR>60或<60ml/min/1.73m²,按1:1随机分为每日一次安慰剂组或非奈利酮10mg或20mg组。主要疗效结局是总eGFR斜率,定义为从基线到第32个月eGFR的年均变化率。次要疗效结局包括一个心肾复合结局,包括肾衰竭时间、eGFR持续下降≥57%、因心力衰竭住院或心血管死亡,以及单独的肾脏和心血管复合结局。记录不良事件以评估耐受性和安全性。
在24个国家,3231名患者接受了筛查,1584名患者被随机分配接受研究治疗。CKD最常见的病因是慢性肾小球肾炎(57.0%)和高血压/缺血性肾病(29.0%)。免疫球蛋白A肾病是最常见的肾小球肾炎(占总人口的26.3%)。基线时,平均eGFR和中位UACR分别为46.7ml/min/1.73m²和818.9mg/g。282名参与者(17.8%)使用了利尿剂,851名(53.7%)使用了他汀类药物,794名(50.1%)使用了钙通道阻滞剂。16.9%的患者使用了钠-葡萄糖协同转运蛋白2(SGLT2)抑制剂;与基线时未使用SGLT2抑制剂的患者相比,这些患者的平均eGFR相似(45.6对46.8ml/min/1.73m²),中位UACR略高(871.9对808.3mg/g)。
FIND-CKD是首个针对非糖尿病病因的CKD患者的非奈利酮3期试验。