Harvard University, Cambridge, MA, United States.
University of North Carolina at Chapel Hill, Chapel Hill, NC, United States.
Econ Hum Biol. 2024 Aug;54:101403. doi: 10.1016/j.ehb.2024.101403. Epub 2024 May 25.
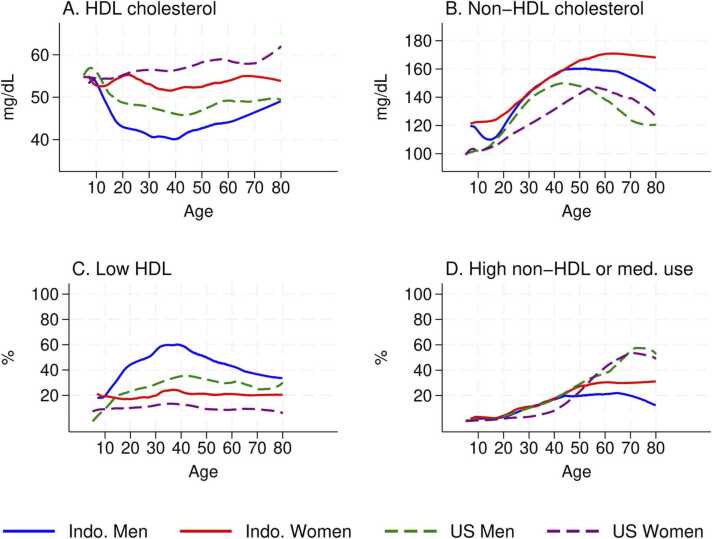
Cardiovascular disease is among the most common causes of death around the world. As rising incomes in low and middle-income countries are accompanied by increased obesity, the burden of disease shifts towards non-communicable diseases, and lower-income settings make up a growing share of cardiovascular disease deaths. Comparative investigation of the roles of body composition, behavioral and socioeconomic factors across countries can shed light on both the biological and social drivers of cardiovascular disease more broadly. Comparing rigorously-validated measures of HDL and non-HDL cholesterol among adults in the United States and in Aceh, Indonesia, we show that Indonesians present with adverse cholesterol biomarkers relative to Americans, despite being younger and having lower body mass index. Adjusting for age, the gaps increase. Body composition, behaviors, demographic and socioeconomic characteristics that affect cholesterol do not explain between-country HDL differences, but do explain non-HDL differences, after accounting for medication use. On average, gender differences are inconsistent across the two countries and persist after controlling observed characteristics. Leveraging the richness of the Indonesian data to draw comparisons of males and females within the same household, the gender gaps among Indonesians are not explained for HDL cholesterol but attenuated substantially for non-HDL cholesterol. This finding suggests that unmeasured household resources play an important role in determining non-HDL cholesterol. More generally, they appear to be affected by social and biological forces in complex ways that differ across countries and potentially operate differently for HDL and non-HDL biomarkers. These results point to the value of rigorous comparative studies to advance understanding of cardiovascular risks across the globe.
心血管疾病是全球最常见的死亡原因之一。随着低收入和中等收入国家收入的增加伴随着肥胖的增加,疾病负担转向非传染性疾病,而低收入环境在心血管疾病死亡中所占的比例越来越大。对各国身体成分、行为和社会经济因素的作用进行比较研究,可以更全面地了解心血管疾病的生物学和社会驱动因素。我们比较了美国和印度尼西亚亚齐成年人经过严格验证的高密度脂蛋白(HDL)和非高密度脂蛋白(non-HDL)胆固醇测量值,结果表明,尽管印度尼西亚人比美国人年轻,体重指数更低,但他们的胆固醇生物标志物却较差。调整年龄后,差距会增大。影响胆固醇的身体成分、行为、人口统计学和社会经济特征不能解释国家间 HDL 的差异,但在考虑药物使用后,可以解释非 HDL 的差异。平均而言,两国的性别差异不一致,并且在控制了观察到的特征后仍然存在。利用印度尼西亚数据的丰富性,对同一家庭内的男性和女性进行比较,印度尼西亚人的性别差距在 HDL 胆固醇方面无法解释,但在非 HDL 胆固醇方面大大减弱。这一发现表明,未被测量的家庭资源在决定非 HDL 胆固醇方面发挥了重要作用。更普遍的是,它们似乎受到社会和生物力量的复杂影响,这些影响在国家之间存在差异,并且对 HDL 和非 HDL 生物标志物的影响可能不同。这些结果表明,严格的比较研究对于提高对全球心血管风险的认识具有重要价值。