Van Haren Robert M, Kovacic Melinda Butsch, Delman Aaron M, Pratt Catherine G, Griffith Azante, Arbili Lana, Harvey Krysten, Kohli Eshika, Pai Ahna, Topalian Alique, Rai Shesh N, Shah Shimul A, Kues John
University of Cincinnati Cancer Center, University of Cincinnati College of Medicine, Cincinnati, OH, USA.
Department of Rehabilitation, Exercise, and Nutrition Sciences, University of Cincinnati College of Allied Health Sciences, Cincinnati, OH, USA.
Ann Surg Oncol. 2024 Sep;31(9):5757-5764. doi: 10.1245/s10434-024-15610-4. Epub 2024 Jun 13.
Underrepresented minority patients with surgical malignancies experience disparities in outcomes. The impact of provider-based factors, including communication, trust, and cultural competency, on outcomes is not well understood. This study examines modifiable provider-based barriers to care experienced by patients with surgical malignancies.
A parallel, prospective, mixed-methods study enrolled patients with lung or gastrointestinal malignancies undergoing surgical consultation. Surveys assessed patients' social needs and patient-physician relationship. Semi-structured interviews ascertained patient experiences and were iteratively analyzed, identifying key themes.
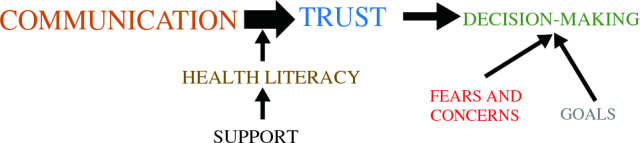
The cohort included 24 patients (age 62 years; 63% White and 38% Black/African American). The most common cancers were lung (n = 18, 75%) and gastroesophageal (n = 3, 13%). Survey results indicated that food insecurity (n = 5, 21%), lack of reliable transportation (n = 4, 17%), and housing instability (n = 2, 8%) were common. Lack of trust in their physician (n = 3, 13%) and their physician's treatment recommendation (n = 3, 13%) were identified. Patients reported a lack of empathy (n = 3, 13%), lack of cultural competence (n = 3, 13%), and inadequate communication (n = 2, 8%) from physicians. Qualitative analysis identified five major themes regarding the decision to undergo surgery: communication, trust, health literacy, patient fears, and decision-making strategies. Five patients (21%) declined the recommended surgery and were more likely Black (100% vs. 21%), lower income (100% vs. 16%), and reported poor patient-physician relationship (40% vs. 5%; all p < 0.05).
Factors associated with declining recommended cancer surgery were underrepresented minority race and poor patient-physician relationships. Interventions are needed to improve these barriers to care and racial disparities.
患有外科恶性肿瘤的少数族裔患者在治疗结果上存在差异。基于医疗服务提供者的因素,包括沟通、信任和文化能力,对治疗结果的影响尚未得到充分理解。本研究探讨了患有外科恶性肿瘤的患者在基于医疗服务提供者方面可改变的护理障碍。
一项平行、前瞻性、混合方法研究纳入了正在接受手术咨询的肺癌或胃肠道恶性肿瘤患者。调查评估了患者的社会需求和医患关系。半结构化访谈确定了患者的经历,并进行了迭代分析,确定了关键主题。
该队列包括24名患者(年龄62岁;63%为白人,38%为黑人/非裔美国人)。最常见的癌症是肺癌(n = 18,75%)和胃食管癌(n = 3,13%)。调查结果表明,粮食不安全(n = 5,21%)、缺乏可靠的交通工具(n = 4,17%)和住房不稳定(n = 2,8%)很常见。患者表示对医生缺乏信任(n = 3,13%)以及对医生的治疗建议缺乏信任(n = 3,13%)。患者报告医生缺乏同理心(n = 3,13%)、缺乏文化能力(n = 3,13%)以及沟通不足(n = 2,8%)。定性分析确定了关于手术决策的五个主要主题:沟通、信任、健康素养、患者恐惧和决策策略。五名患者(21%)拒绝了推荐的手术,他们更可能是黑人(100%对21%)、收入较低(100%对16%),并且报告医患关系较差(40%对5%;所有p < 0.05)。
与拒绝推荐的癌症手术相关的因素是少数族裔以及不良的医患关系。需要采取干预措施来改善这些护理障碍和种族差异。