Department of Orthopedic Surgery, Kitasato University School of Medicine, 1-15-1 Kitasato, Minami-Ku, Sagamihara City, Kanagawa, 252-0374, Japan.
Department of Physical Therapy, Fukushima Medical University School of Health Sciences, 10-6 Sakaemachi, Fukushima City, Fukushima, 960-8516, Japan.
BMC Musculoskelet Disord. 2024 Jun 18;25(1):475. doi: 10.1186/s12891-024-07604-w.
Suction drainages are commonly used after total knee arthroplasty (TKA) procedures; however, their use is somewhat controversial. Recently, some reports have claimed that the administration of tranexamic acid (TXA) may prevent postoperative bleeding following TKAs. Although numerous studies have reported regarding different dosages, timings of administration, or drain clamping times for intravenous and intra-articular TXA injections (IA-TXAs), few have examined whether suction drainage is necessary when TXA is administered. In this study, we compared using suction drainage without TXA administration and IA-TXA without suction drainage and aimed to examine the need for suction drainage during IA-TXA.
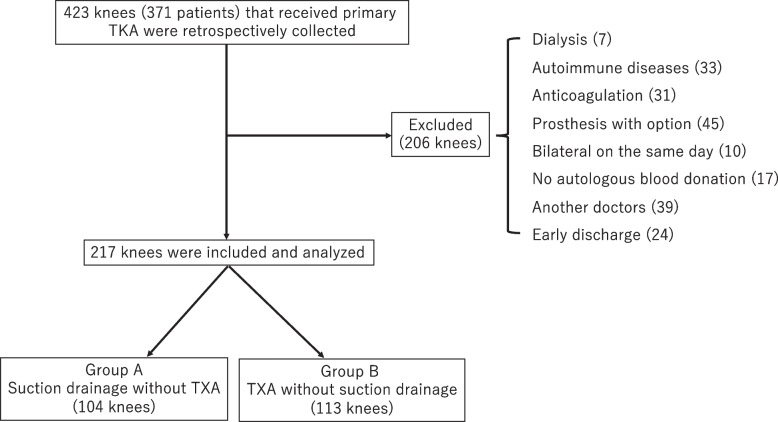
This retrospective study was conducted on 217 patients who had received TKA for osteoarthritis; 104 were placed on suction drainage after TKA without TXA (Group A), whereas the remaining 113 received IA-TXA immediately after surgery without suction drainage (Group B). Our clinical evaluation included assessments of the need for transfusion, presence of postoperative complications, incidence of deep vein thrombosis (DVT), and changes in hemoglobin (Hb), hematocrit (Hct), and D-dimer levels.
No significant differences were observed in terms of postoperative complications and preoperative Hb, Hct, or D-dimer levels between the two groups. Although the prevalence of DVT was significantly higher in Group B (p < 0.05), all cases were asymptomatic. Hb and Hct levels were significantly lower in Group A than in Group B at 1, 3, 7, and 14 days postoperatively (p < 0.05), although none of the cases required blood transfusions. D-dimer levels were significantly higher in Group A than in Group B at 1 and 3 days postoperatively (p < 0.05).
Suction drainage might not be necessary when IA-TXA is administered after TKA procedures.
膝关节置换术后(TKA)常使用引流管,但引流的使用存在一定争议。最近有报道称,使用氨甲环酸(TXA)可能会减少 TKA 术后出血。虽然有许多研究报道了不同剂量、给药时间或静脉内和关节内 TXA 注射(IA-TXAs)的引流夹闭时间,但很少有研究探讨 TXA 给药时是否需要引流。在这项研究中,我们比较了 TKA 后不使用 TXA 引流和立即使用 IA-TXA 且不使用引流的情况,并旨在探讨 IA-TXA 时是否需要引流。
这是一项回顾性研究,纳入了 217 例因骨关节炎行 TKA 的患者;104 例 TKA 后未使用 TXA 但放置了引流管(A 组),其余 113 例在手术后立即接受 IA-TXA 且未放置引流管(B 组)。我们的临床评估包括输血需求、术后并发症、深静脉血栓形成(DVT)发生率以及血红蛋白(Hb)、红细胞压积(Hct)和 D-二聚体水平的变化。
两组患者在术后并发症、术前 Hb、Hct 或 D-二聚体水平方面无显著差异。虽然 B 组 DVT 的发生率显著更高(p < 0.05),但所有病例均无症状。与 B 组相比,A 组在术后 1、3、7 和 14 天的 Hb 和 Hct 水平显著更低(p < 0.05),但均未输血。A 组在术后 1 和 3 天的 D-二聚体水平显著更高(p < 0.05)。
TKA 后行 IA-TXA 时可能不需要引流。