Wang Jade, O'Dwyer Elisabeth, Martinez Zuloaga Juana, Subramanian Kritika, Hu Jim C, Jhanwar Yuliya S, Nagar Himanshu, RoyChoudhury Arindam, Babich John, Huicochea Castellanos Sandra, Osborne Joseph R, Margolis Daniel J A
Department of Internal Medicine, New York-Presbyterian Hospital, New York, NY 10065, USA.
Department of Radiology, Weill Cornell Medical College, New York, NY 10065, USA.
Cancers (Basel). 2024 May 29;16(11):2056. doi: 10.3390/cancers16112056.
PSMA PET has emerged as a "gold standard" imaging modality for assessing prostate cancer metastases. However, it is not universally available, and this limits its impact. In contrast, whole-body MRI is much more widely available but misses more lesions. This study aims to improve the interpretation of whole-body MRI by comparing false negative scans retrospectively to PSMA PET.
This study was a retrospective sub-analysis of a prospectively collected database of patients who participated in a clinical trial of PSMA PET/MRI comparing PSMA PET and whole-body MRI from 2018-2021. Subjects whose separately read PSMA PET and MRI diagnostic reports showed discrepancies ("false negative" MRI cases) were selected for sub-analysis. The cases were reviewed by the same attending radiologist who originally read the scans. The radiologist noted specific features on MRI indicating metastatic disease that were initially missed.
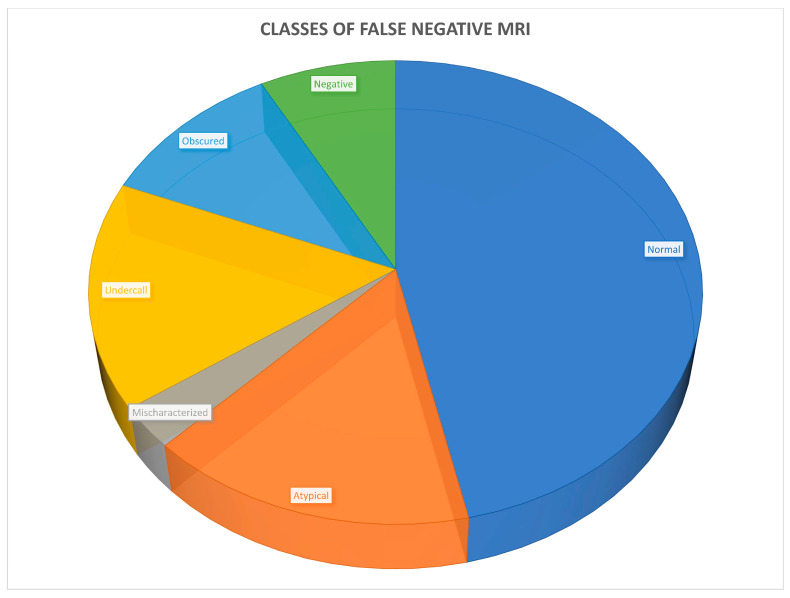
Of 263 cases, 38 (14%) met the inclusion criteria and were reviewed. Six classes of mpMRI false negatives were identified: anatomically normal (18, 47%), atypical MRI appearance (6, 16%), mischaracterization (1, 3%), undercall (6, 16%), obscured (4, 11%), and no abnormality on MRI (3, 8%). Considering that the atypical and undercalled cases could have been adjusted in retrospect, and that 4 additional cases had positive lesions to the same extent and 11 further cases had disease confined to the pelvis, only 11 (4%) of the original 263 would have had disease outside of a conventional radiation treatment plan.
Notably, almost 50% of the cases, including most lymph node metastases, were anatomically normal using standard criteria. This suggests that current anatomic criteria for evaluating prostate cancer lymph node metastases are not ideal, and there is a need for improved criteria. In addition, 32% of cases involved some element of human interpretive error, and, therefore, improving reader training may lead to more accurate results.
前列腺特异性膜抗原(PSMA)正电子发射断层扫描(PET)已成为评估前列腺癌转移的“金标准”成像方式。然而,它并非普遍可用,这限制了其影响力。相比之下,全身磁共振成像(MRI)的可用性要广泛得多,但会遗漏更多病灶。本研究旨在通过将假阴性扫描结果与PSMA PET进行回顾性比较,来改进全身MRI的解读。
本研究是对一个前瞻性收集的患者数据库进行的回顾性子分析,这些患者参与了一项2018 - 2021年比较PSMA PET和全身MRI的PSMA PET/MRI临床试验。选择那些单独阅读的PSMA PET和MRI诊断报告显示存在差异(“假阴性”MRI病例)的受试者进行子分析。这些病例由最初阅读扫描结果的同一位主治放射科医生进行复查。放射科医生记录了MRI上最初遗漏的表明转移性疾病的特定特征。
在263例病例中,38例(14%)符合纳入标准并接受了复查。确定了六类多参数磁共振成像(mpMRI)假阴性:解剖结构正常(18例,47%)、MRI表现不典型(6例,16%)、误诊(1例,3%)、漏诊(6例,16%)、病灶模糊(4例,11%)以及MRI无异常(3例,8%)。考虑到不典型和漏诊的病例在回顾时可能已得到调整,并且另外有4例病例有同等程度的阳性病灶,还有11例病例疾病局限于盆腔,那么在最初的263例病例中,只有11例(4%)会有超出传统放射治疗计划范围的疾病。
值得注意的是,几乎50%的病例,包括大多数淋巴结转移,按照标准标准解剖结构是正常的。这表明当前评估前列腺癌淋巴结转移的解剖学标准并不理想,需要改进标准。此外,32%的病例存在人为解读错误的因素,因此,改进阅片者培训可能会带来更准确的结果。