Study Group of Diabetology of the Italian Society for Pediatric Endocrinology and Diabetes (I.S.P.E.D.,) University Hospital of Ferrara, Ferrara, Italy.
Department of Maternal and Child Health, UOSD Regional Center of Pediatric Diabetology, Annunziata Hospital, Chieti, Italy.
Front Endocrinol (Lausanne). 2024 Jun 4;15:1387537. doi: 10.3389/fendo.2024.1387537. eCollection 2024.
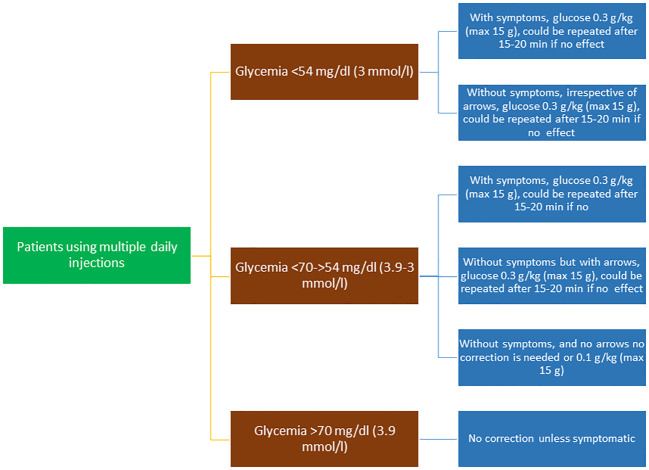
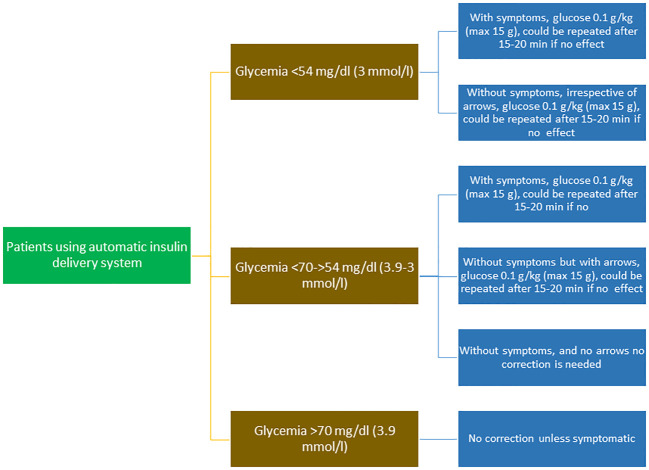
There has been continuous progress in diabetes management over the last few decades, not least due to the widespread dissemination of continuous glucose monitoring (CGM) and automated insulin delivery systems. These technological advances have radically changed the daily lives of people living with diabetes, improving the quality of life of both children and their families. Despite this, hypoglycemia remains the primary side-effect of insulin therapy. Based on a systematic review of the available scientific evidence, this paper aims to provide evidence-based recommendations for recognizing, risk stratifying, treating, and managing patients with hypoglycemia. The objective of these recommendations is to unify the behavior of pediatric diabetologists with respect to the timely recognition and prevention of hypoglycemic episodes and the correct treatment of hypoglycemia, especially in patients using CGM or advanced hybrid closed-loop systems. All authors have long experience in the specialty and are members of the Italian Society of Pediatric Endocrinology and Diabetology. The goal of treating hypoglycemia is to raise blood glucose above 70 mg/dL (3.9 mmol/L) and to prevent further decreases. Oral glucose at a dose of 0.3 g/kg (0.1 g/kg for children using "smart pumps" or hybrid closed loop systems in automated mode) is the preferred treatment for the conscious individual with blood glucose <70 mg/dL (3.9 mmol/L), although any form of carbohydrate (e.g., sucrose, which consists of glucose and fructose, or honey, sugary soft drinks, or fruit juice) containing glucose may be used. Using automatic insulin delivery systems, the oral glucose dose can be decreased to 0.1 g/kg. Practical flow charts are included to aid clinical decision-making. Although representing the official position of the Italian Society of Pediatric Endocrinology and Diabetology (ISPED), these guidelines are applicable to the global audience and are especially pertinent in the era of CGM and other advanced technologies.
在过去的几十年中,糖尿病管理取得了持续的进展,这主要得益于连续血糖监测(CGM)和自动胰岛素输送系统的广泛传播。这些技术进步彻底改变了糖尿病患者的日常生活,提高了儿童及其家庭的生活质量。尽管如此,低血糖仍然是胰岛素治疗的主要副作用。基于对现有科学证据的系统回顾,本文旨在为识别、风险分层、治疗和管理低血糖患者提供循证建议。这些建议的目的是统一儿科内分泌学家对及时识别和预防低血糖发作以及正确治疗低血糖的行为,特别是在使用 CGM 或先进的混合闭环系统的患者中。所有作者在该专业领域都拥有丰富的经验,并且都是意大利儿科内分泌学会和糖尿病学会的成员。治疗低血糖的目标是将血糖升高到 70mg/dL(3.9mmol/L)以上,并防止进一步下降。对于血糖<70mg/dL(3.9mmol/L)的意识清醒的个体,首选口服 0.3g/kg 的葡萄糖(使用“智能泵”或混合闭环系统自动模式的儿童为 0.1g/kg),尽管任何形式的碳水化合物(例如由葡萄糖和果糖组成的蔗糖,或蜂蜜、含糖软饮料或果汁)都含有葡萄糖,都可以使用。使用自动胰岛素输送系统,口服葡萄糖剂量可减少至 0.1g/kg。本文还包含了实用的流程图,以帮助临床决策。尽管这些指南代表了意大利儿科内分泌学会和糖尿病学会(ISPED)的官方立场,但它们适用于全球受众,尤其是在 CGM 和其他先进技术时代。