Department of Circulation and Medical Imaging, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology (NTNU), 7491, Trondheim, Norway.
Department of Radiology, Vestre Viken Hospital Trust, Drammen Hospital, 3004, Drammen, Norway.
Eur Radiol. 2024 Dec;34(12):8015-8029. doi: 10.1007/s00330-024-10841-1. Epub 2024 Jun 19.
We analysed magnetic resonance imaging (MRI) findings after traumatic brain injury (TBI) aiming to improve the grading of traumatic axonal injury (TAI) to better reflect the outcome.
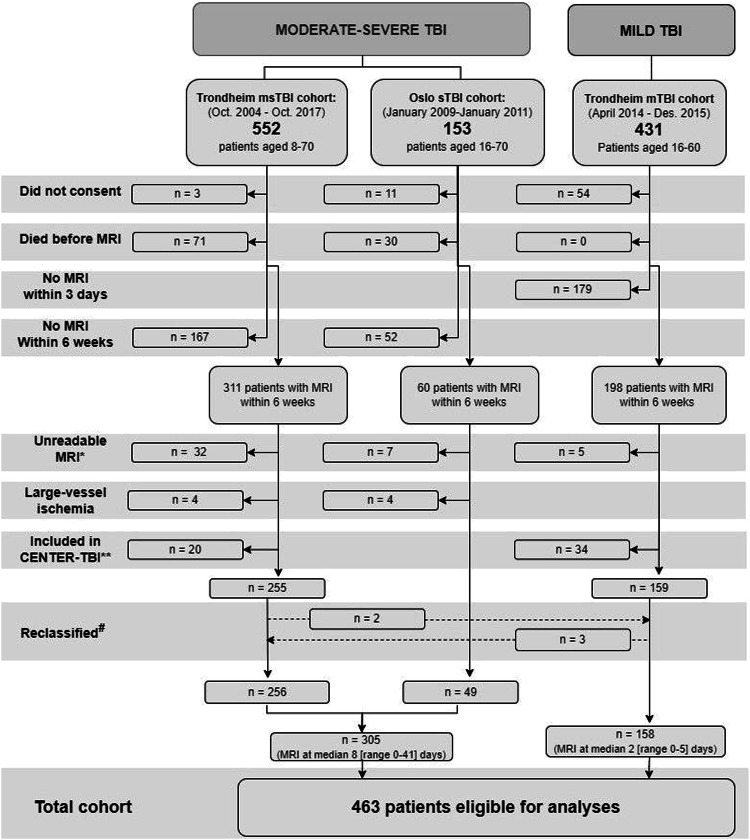
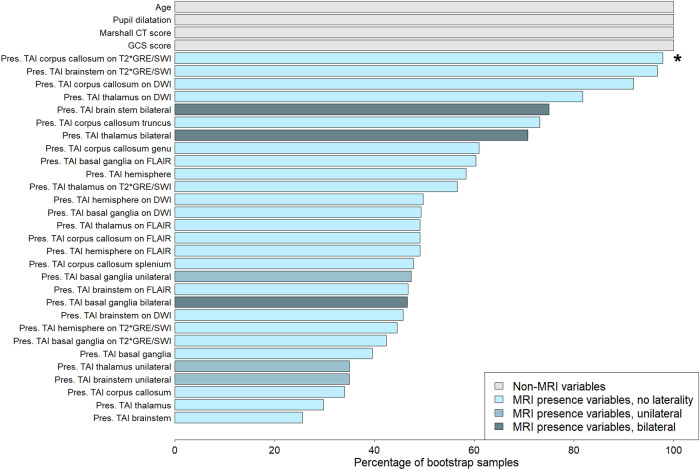
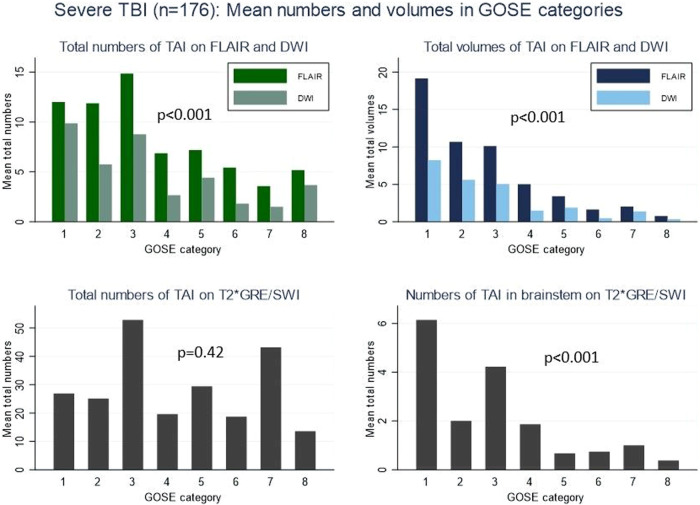
Four-hundred sixty-three patients (8-70 years) with mild (n = 158), moderate (n = 129), or severe (n = 176) TBI and early MRI were prospectively included. TAI presence, numbers, and volumes at predefined locations were registered on fluid-attenuated inversion recovery (FLAIR) and diffusion-weighted imaging, and presence and numbers on T2*GRE/SWI. Presence and volumes of contusions were registered on FLAIR. We assessed the outcome with the Glasgow Outcome Scale Extended. Multivariable logistic and elastic-net regression analyses were performed.
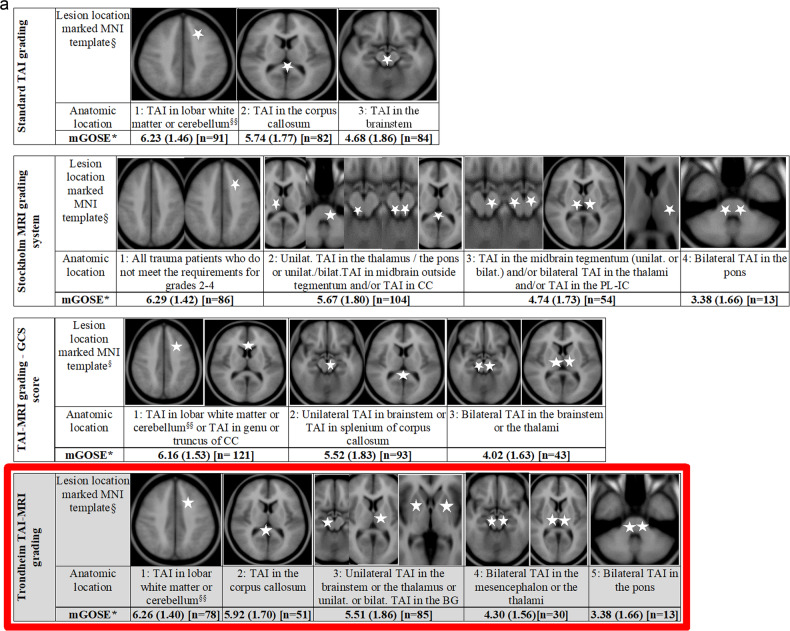
The presence of TAI differed between mild (6%), moderate (70%), and severe TBI (95%). In severe TBI, bilateral TAI in mesencephalon or thalami and bilateral TAI in pons predicted worse outcomes and were defined as the worst grades (4 and 5, respectively) in the Trondheim TAI-MRI grading. The Trondheim TAI-MRI grading performed better than the standard TAI grading in severe TBI (pseudo-R 0.19 vs. 0.16). In moderate-severe TBI, quantitative models including both FLAIR volume of TAI and contusions performed best (pseudo-R 0.19-0.21). In patients with mild TBI or Glasgow Coma Scale (GCS) score 13, models with the volume of contusions performed best (pseudo-R 0.25-0.26).
We propose the Trondheim TAI-MRI grading (grades 1-5) with bilateral TAI in mesencephalon or thalami, and bilateral TAI in pons as the worst grades. The predictive value was highest for the quantitative models including FLAIR volume of TAI and contusions (GCS score <13) or FLAIR volume of contusions (GCS score ≥ 13), which emphasise artificial intelligence as a potentially important future tool.
The Trondheim TAI-MRI grading reflects patient outcomes better in severe TBI than today's standard TAI grading and can be implemented after external validation. The prognostic importance of volumetric models is promising for future use of artificial intelligence technologies.
Traumatic axonal injury (TAI) is an important injury type in all TBI severities. Studies demonstrating which MRI findings that can serve as future biomarkers are highly warranted. This study proposes the most optimal MRI models for predicting patient outcome at 6 months after TBI; one updated pragmatic model and a volumetric model. The Trondheim TAI-MRI grading, in severe TBI, reflects patient outcome better than today's standard grading of TAI and the prognostic importance of volumetric models in all severities of TBI is promising for future use of AI.
我们分析了外伤性脑损伤(TBI)后的磁共振成像(MRI)结果,旨在改善外伤性轴索损伤(TAI)的分级,以更好地反映结果。
前瞻性纳入了 463 例(8-70 岁)轻度(n=158)、中度(n=129)或重度(n=176)TBI 且早期 MRI 患者。在液体衰减反转恢复(FLAIR)和弥散加权成像上记录 TAI 的存在、数量和体积,在 T2*GRE/SWI 上记录 TAI 的存在和数量。在 FLAIR 上记录挫伤的存在和体积。我们使用格拉斯哥预后量表扩展版评估了预后。进行了多变量逻辑和弹性网回归分析。
在轻度(6%)、中度(70%)和重度 TBI(95%)中,TAI 的存在存在差异。在重度 TBI 中,中脑或丘脑的双侧 TAI 和脑桥的双侧 TAI 预测预后更差,分别被定义为 Trondheim TAI-MRI 分级的最差等级(分别为 4 级和 5 级)。在重度 TBI 中,Trondheim TAI-MRI 分级的表现优于标准 TAI 分级(伪 R 0.19 与 0.16)。在中重度 TBI 中,包括 FLAIR 上 TAI 体积和挫伤的定量模型表现最佳(伪 R 0.19-0.21)。在轻度 TBI 或格拉斯哥昏迷量表(GCS)评分 13 的患者中,包含挫伤体积的模型表现最佳(伪 R 0.25-0.26)。
我们提出了 Trondheim TAI-MRI 分级(1-5 级),中脑或丘脑的双侧 TAI 和脑桥的双侧 TAI 为最差等级。包括 FLAIR 上 TAI 体积和挫伤的定量模型或 FLAIR 上挫伤体积(GCS 评分≥13)的预测价值最高,这强调了人工智能作为一种潜在的重要未来工具。
与目前的标准 TAI 分级相比,Trondheim TAI-MRI 分级在重度 TBI 中能更好地反映患者预后,且可在外部验证后实施。容积模型的预后重要性为未来使用人工智能技术提供了希望。
外伤性轴索损伤(TAI)是所有 TBI 严重程度中的一种重要损伤类型。迫切需要研究证明哪些 MRI 发现可以作为未来的生物标志物。本研究提出了预测 TBI 后 6 个月患者预后的最佳 MRI 模型;一个更新的实用模型和一个体积模型。在重度 TBI 中,Trondheim TAI-MRI 分级比目前的 TAI 分级更能反映患者的预后,且所有严重程度的 TBI 中容积模型的预后重要性对未来人工智能的应用具有很大的潜力。