Cejka Daniel, Thiem Ursula, Blinzler Eric, Machacek Jennifer, Voelkl Jakob, Smith Edward R, Pasch Andreas, Haller Maria C
Department of Medicine III - Nephrology, Hypertension, Transplantation, Rheumatology, Geriatrics, Ordensklinikum Linz - Elisabethinen Hospital, Linz, Austria.
Faculty of Medicine, Johannes Kepler University Linz, Austria.
Kidney Int Rep. 2024 Mar 25;9(6):1765-1773. doi: 10.1016/j.ekir.2024.03.023. eCollection 2024 Jun.
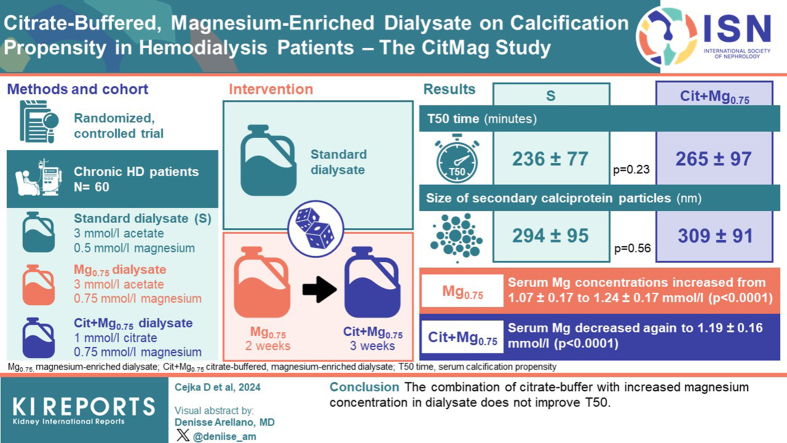
Serum calcification propensity (T50 time) is associated with mortality in patients on dialysis. Several solitary interventions improve T50. However, whether a combination of interventions yields further increases in T50 is unknown. We hypothesized that a combination of 2 interventions, namely increasing magnesium concentration while simultaneously substituting acetate for citrate in the dialysis fluid, leads to increases in T50 values.
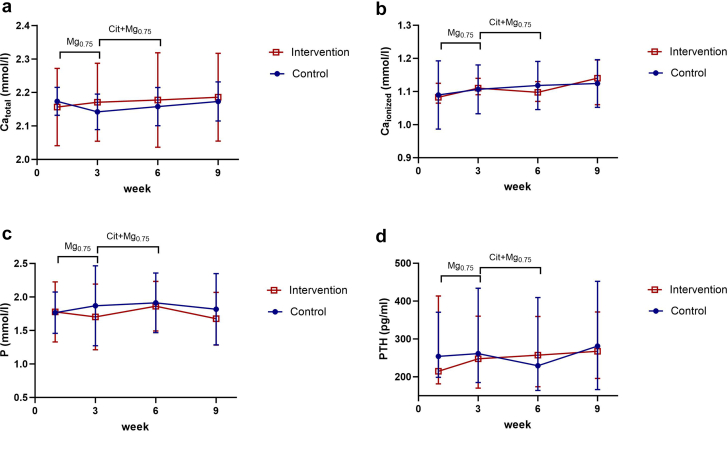
In a randomized controlled trial, 60 patients on chronic hemodialysis were allocated to either continue on standard (S) dialysate (3 mmol/l acetate, 0.5 mmol/l magnesium) or a sequence of magnesium-enriched (Mg) dialysate (3 mmol/l acetate, 0.75 mmol/l magnesium) for 2 weeks followed by combination treatment using citrate-buffered, magnesium-enriched (Cit+Mg) dialysate (1 mmol/l citrate, 0.75 mmol/l magnesium) for 3 weeks. The primary end point was the difference in T50 times between the S group and the Cit+Mg group.
There was no significant difference in T50 time between the S group and the Cit+Mg group (236 ± 77 vs. 265 ± 97 min, = 0.23). The size (hydrodynamic radius) of secondary calciprotein particles did not differ between the S group and the Cit+Mg group (294 ± 95 vs. 309 ± 91 nm, = 0.56). In longitudinal analyses, serum magnesium concentrations increased from 1.07 ± 0.17 to 1.24 ± 0.17 mmol/l with the Mg dialysate ( < 0.0001) but decreased again to 1.19 ± 0.16 mmol/l with the Cit+Mg dialysate ( < 0.0001).
The combination of citrate buffer with increased magnesium concentration in dialysate does not improve T50.
血清钙化倾向(T50时间)与透析患者的死亡率相关。几种单独的干预措施可改善T50。然而,联合干预是否会进一步提高T50尚不清楚。我们假设两种干预措施联合使用,即在透析液中提高镁浓度并同时用醋酸盐替代柠檬酸盐,会导致T50值增加。
在一项随机对照试验中,60例慢性血液透析患者被分配继续使用标准(S)透析液(3 mmol/L醋酸盐,0.5 mmol/L镁)或使用富含镁(Mg)的透析液(3 mmol/L醋酸盐,0.75 mmol/L镁)2周,随后使用柠檬酸盐缓冲的富含镁(Cit+Mg)的透析液(1 mmol/L柠檬酸盐,0.75 mmol/L镁)联合治疗3周。主要终点是S组和Cit+Mg组之间T50时间的差异。
S组和Cit+Mg组之间的T50时间无显著差异(236±77 vs. 265±97分钟,P = 0.23)。S组和Cit+Mg组之间二级钙化蛋白颗粒的大小(流体动力学半径)无差异(294±95 vs. 309±91 nm,P = 0.56)。在纵向分析中,使用Mg透析液时血清镁浓度从1.07±0.17 mmol/L增加到1.24±0.17 mmol/L(P<0.0001),但使用Cit+Mg透析液时又降至1.19±0.16 mmol/L(P<0.0001)。
透析液中柠檬酸盐缓冲液与增加的镁浓度联合使用并不能改善T50。