Department of Cancer Pharmacology & Pharmacogenomics, Atrium Health Levine Cancer Institute, Charlotte, NC.
Molecular Biology and Genomics Core Facility, Atrium Health Levine Cancer Institute, Charlotte, NC.
JCO Precis Oncol. 2024 Jun;8:e2300623. doi: 10.1200/PO.23.00623.
Fluoropyrimidine-related toxicity and mortality risk increases significantly in patients carrying certain genetic variants with standard dosing. We implemented genotyping at a multisite cancer center and evaluated its impact on dosing, toxicity, and hospitalization.
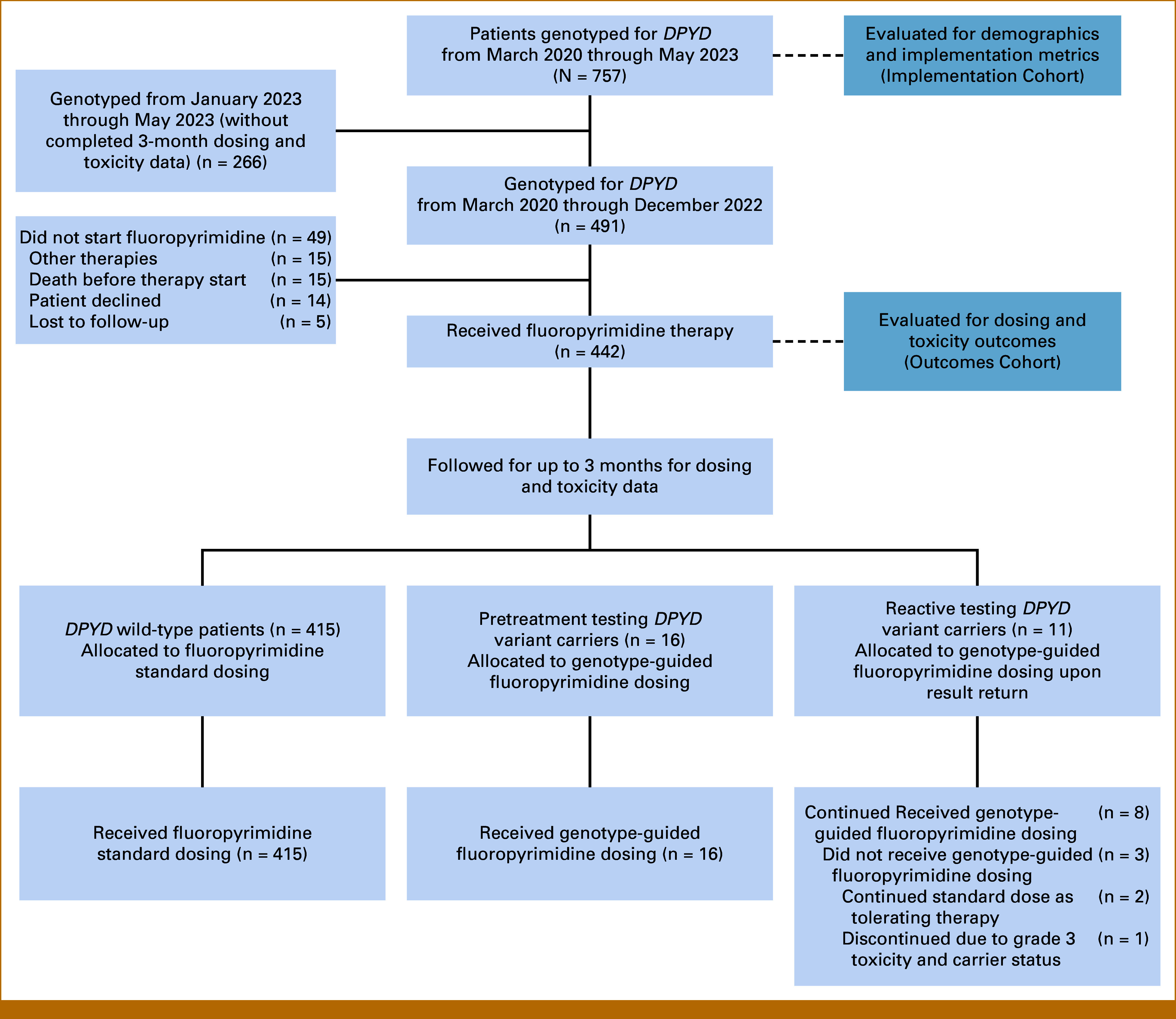
In this prospective observational study, patients receiving (reactive) or planning to receive (pretreatment) fluoropyrimidine-based chemotherapy were genotyped for five variants as standard practice per provider discretion. The primary end point was the proportion of variant carriers receiving fluoropyrimidine modifications. Secondary end points included mean relative dose intensity, fluoropyrimidine-related grade 3+ toxicities, and hospitalizations. Fisher's exact test compared toxicity and hospitalization rates between pretreatment carriers, reactive carriers, and wild-type patients. Univariable and multivariable logistic regression identified factors associated with toxicity and hospitalization risk. Kaplan-Meier methods estimated time to event of first grade 3+ toxicity and hospitalization.
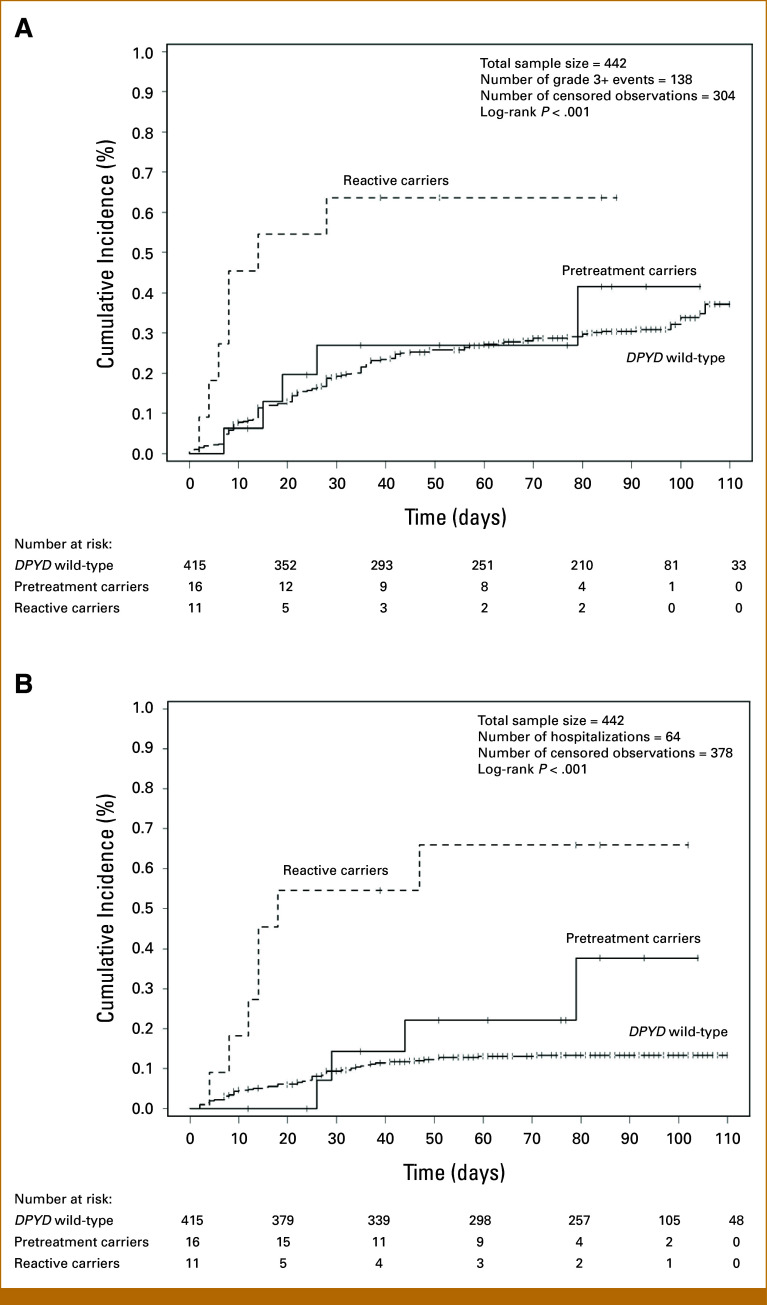
Of the 757 patients who received genotyping (median age 63, 54% male, 74% White, 19% Black, 88% GI malignancy), 45 (5.9%) were heterozygous carriers. Fluoropyrimidine was modified in 93% of carriers who started treatment. In 442 patients with 3-month follow-up, 64%, 31%, and 30% of reactive carriers, pretreatment carriers, and wild-type patients had grade 3+ toxicity, respectively ( = .085); 64%, 25%, and 13% were hospitalized ( < .001). Reactive carriers had 10-fold higher odds of hospitalization compared with wild-type patients ( = .001), whereas no significant difference was noted between pretreatment carriers and wild-type patients. Time-to-event of toxicity and hospitalization were significantly different between genotype groups ( < .001), with reactive carriers having the earliest onset and highest incidence.
genotyping prompted fluoropyrimidine modifications in most carriers. Pretreatment testing reduced toxicities and hospitalizations compared with reactive testing, thus normalizing the risk to that of wild-type patients, and should be considered standard practice.
在接受标准剂量治疗的患者中,携带某些特定基因突变的患者,氟嘧啶类相关毒性和死亡风险显著增加。我们在一个多站点癌症中心实施了基因分型,并评估了其对剂量、毒性和住院治疗的影响。
在这项前瞻性观察性研究中,根据医生的判断,为接受(反应性)或计划接受(预处理)氟嘧啶类化疗的患者进行五种变体的基因分型。主要终点是变体携带者接受氟嘧啶类药物修改的比例。次要终点包括平均相对剂量强度、氟嘧啶类相关 3 级及以上毒性和住院治疗。Fisher 确切检验比较了预处理携带者、反应性携带者和野生型患者之间的毒性和住院治疗率。单变量和多变量逻辑回归确定了与毒性和住院治疗风险相关的因素。Kaplan-Meier 方法估计了首次发生 3 级及以上毒性和住院治疗的时间。
在接受基因分型的 757 例患者中(中位年龄 63 岁,54%为男性,74%为白人,19%为黑人,88%为胃肠道恶性肿瘤),45 例(5.9%)为杂合子携带者。开始治疗的携带者中 93%的人改变了氟嘧啶类药物的使用。在 442 例有 3 个月随访的患者中,反应性携带者、预处理携带者和野生型患者分别有 64%、31%和 30%发生 3 级及以上毒性(=0.085);64%、25%和 13%的患者住院(<0.001)。与野生型患者相比,反应性携带者的住院风险高 10 倍(=0.001),而预处理携带者与野生型患者之间无显著差异。毒性和住院治疗的时间事件在基因型组之间有显著差异(<0.001),反应性携带者的发病最早,发生率最高。
基因分型促使大多数携带者改变了氟嘧啶类药物的使用。与反应性检测相比,预处理检测减少了毒性和住院治疗,从而使风险与野生型患者相同,因此应被视为标准做法。